

Myorelaxants in ARDS patients
- PMID: 33159530
- PMCID: PMC7648542
- DOI: 10.1007/s00134-020-06297-8
Myorelaxants in ARDS patients
Abstract
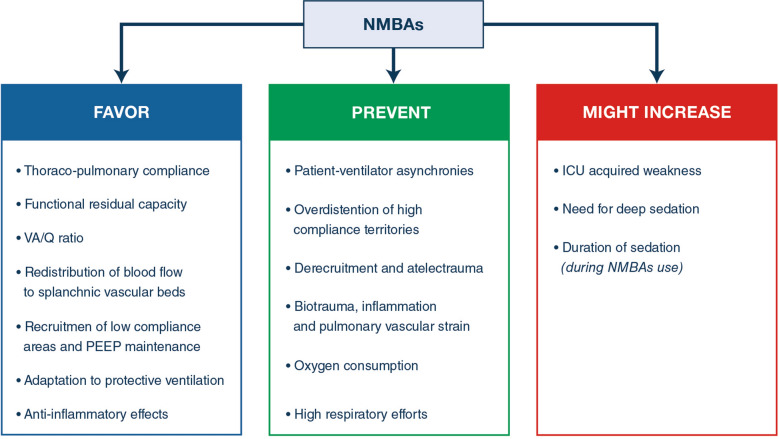
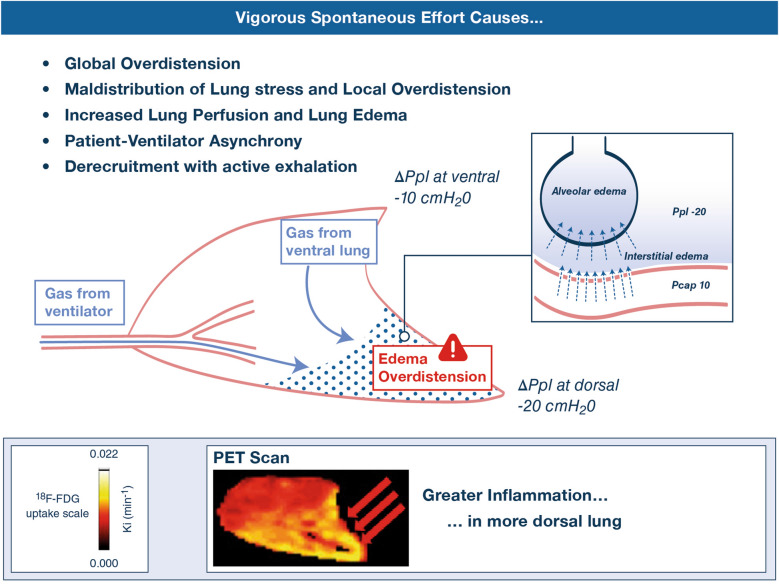
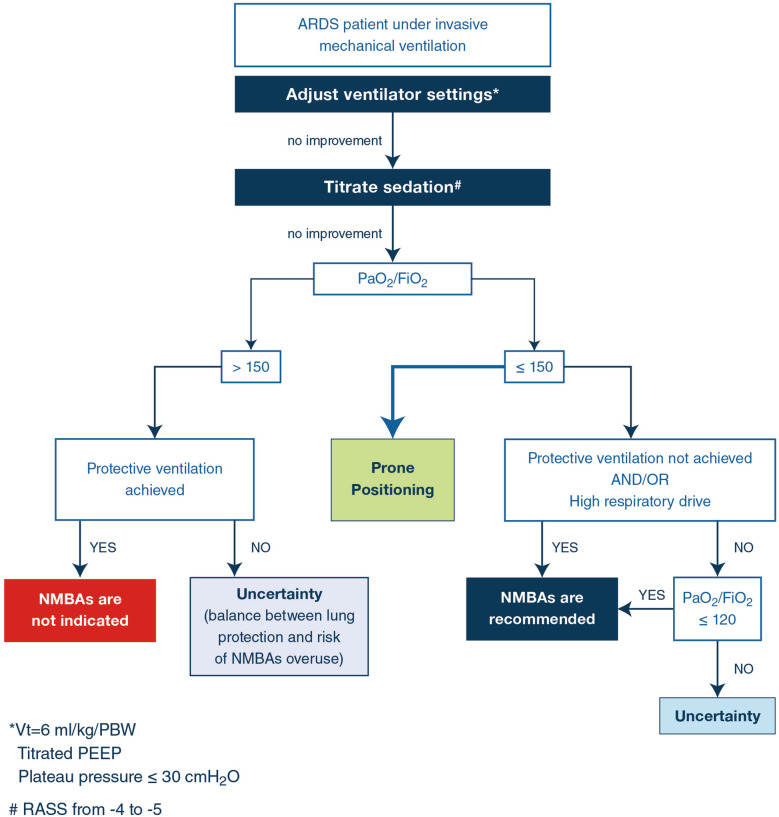
Neuromuscular blocking agents (NMBAs) inhibit patient-initiated active breath and the risk of high tidal volumes and consequent high transpulmonary pressure swings, and minimize patient/ ventilator asynchrony in acute respiratory distress syndrome (ARDS). Minimization of volutrauma and ventilator-induced lung injury (VILI) results in a lower incidence of barotrauma, improved oxygenation and a decrease in circulating proinflammatory markers. Recent randomized clinical trials did not reveal harmful muscular effects during a short course of NMBAs. The use of NMBAs should be considered during the early phase of severe ARDS for patients to facilitate lung protective ventilation or prone positioning only after optimising mechanical ventilation and sedation. The use of NMBAs should be integrated in a global strategy including the reduction of tidal volume, the rational use of PEEP, prone positioning and the use of a ventilatory mode allowing spontaneous ventilation as soon as possible. Partial neuromuscular blockade should be evaluated in future trials.
Keywords: Corticosteroids; ECMO; Muscle relaxants; PEEP; Prone positioning; Protective ventilation; Sedation.
Conflict of interest statement
SH has no conflict of interest. LP received consultancy fees from Air Liquide MS, Faron and MSD. VF has not conflict of interest. LH received a research grant from Liberate Medical, USA and speakers fee from Getinge, Sweden and Liberate Medical, USA. PDS has no conflicts of interest. TY has no conflicts of interest. AG has no conflicts of interest, SJ reports consulting fees from Drager, Fresenius-Xenios, Baxter, Medtronic, and Fisher and Paykel. DA has no conflicts of interest.
Figures
References
-
- Arroliga AC, Thompson BT, Ancukiewicz M, Gonzales JP, Guntupalli KK, Park PK, Wiedemann HP, Anzueto A, Acute Respiratory Distress Syndrome N Use of sedatives, opioids, and neuromuscular blocking agents in patients with acute lung injury and acute respiratory distress syndrome. Crit Care Med. 2008;36:1083–1088. doi: 10.1097/CCM.0B013E3181653895. - DOI - PubMed
-
- Combes A, Hajage D, Capellier G, Demoule A, Lavoue S, Guervilly C, Da Silva D, Zafrani L, Tirot P, Veber B, Maury E, Levy B, Cohen Y, Richard C, Kalfon P, Bouadma L, Mehdaoui H, Beduneau G, Lebreton G, Brochard L, Ferguson ND, Fan E, Slutsky AS, Brodie D, Mercat A, Eolia Trial Group R, Ecmonet Extracorporeal membrane oxygenation for severe acute respiratory distress Syndrome. N Engl J Med. 2018;378:1965–1975. doi: 10.1056/NEJMoa1800385. - DOI - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
