

Discovery, validation and sequencing of urinary peptides for diagnosis of liver fibrosis-A multicentre study
- PMID: 33160210
- PMCID: PMC7648178
- DOI: 10.1016/j.ebiom.2020.103083
Discovery, validation and sequencing of urinary peptides for diagnosis of liver fibrosis-A multicentre study
Abstract
Background: Liver fibrosis is a consequence of chronic inflammation and is associated with protein changes within the hepatocytes structure. In this study, we aimed to investigate if this is reflected by the urinary proteome and can be explored to diagnose liver fibrosis in patients with chronic liver disease.
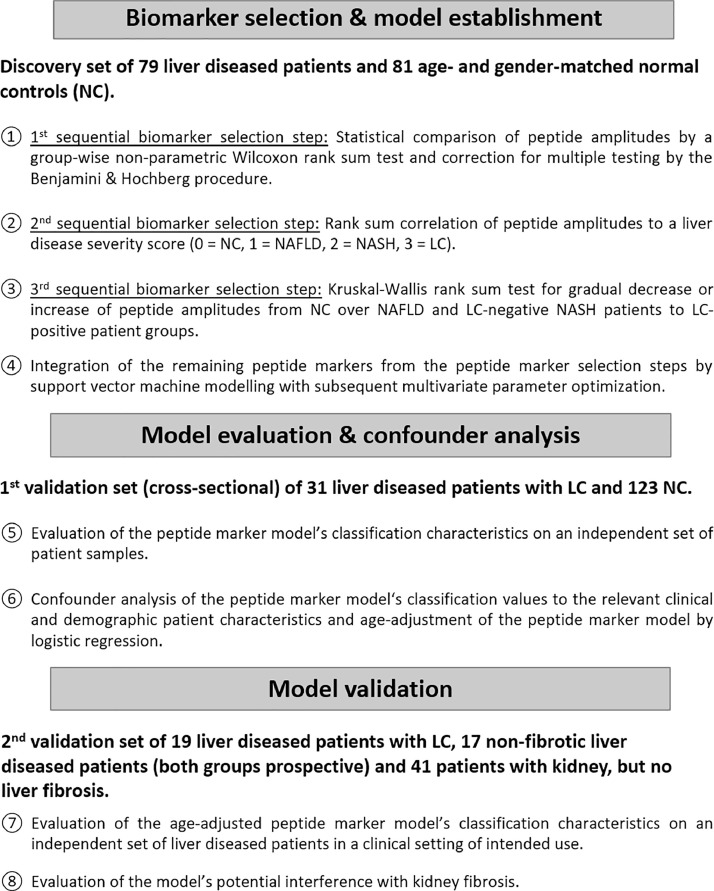
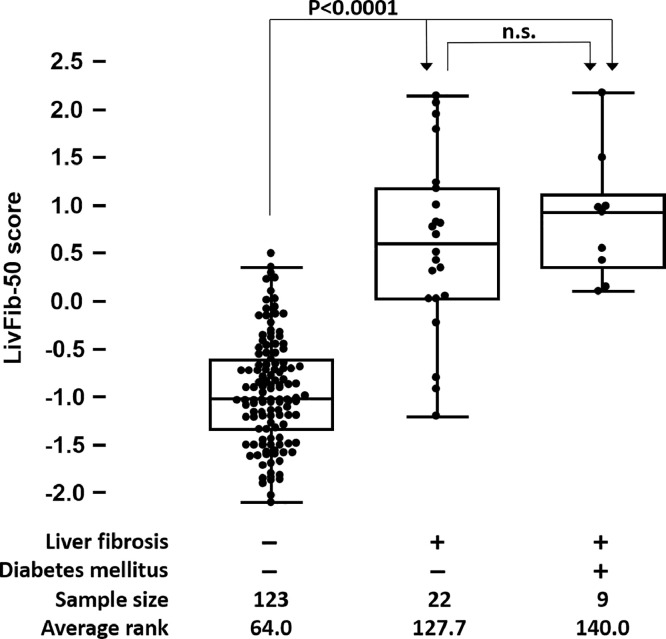
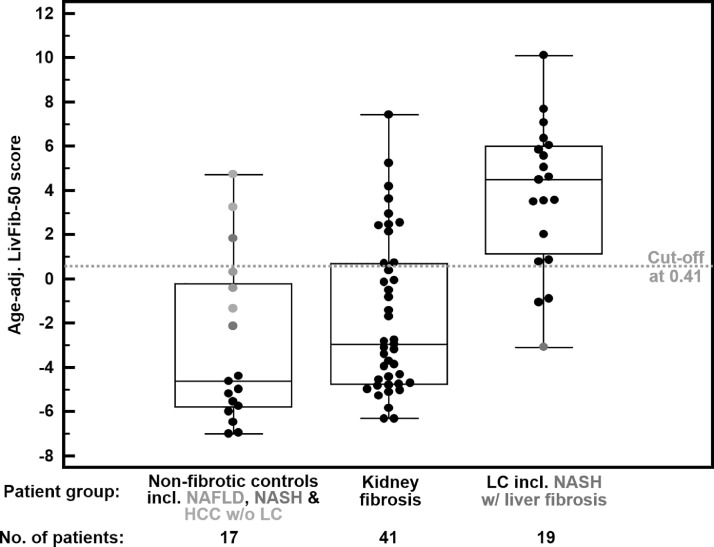
Methods: In a multicentre combined cross-sectional and prospective diagnostic test validation study, 129 patients with varying degrees of liver fibrosis and 223 controls without liver fibrosis were recruited. Additionally, 41 patients with no liver, but kidney fibrosis were included to evaluate interference with expressions of kidney fibrosis. Urinary low molecular weight proteome was analysed by capillary electrophoresis coupled to mass spectrometry (CE-MS) and a support vector machine marker model was established by integration of peptide markers for liver fibrosis.
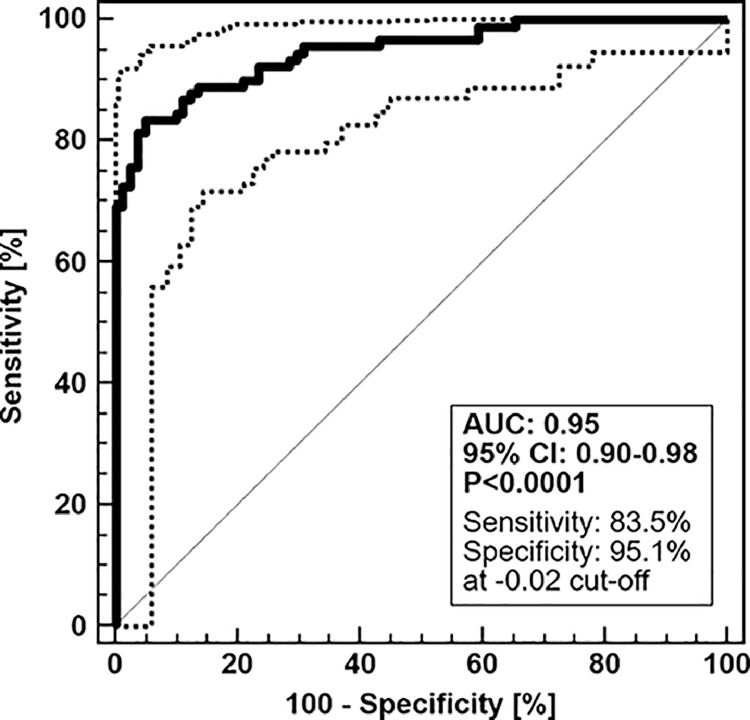
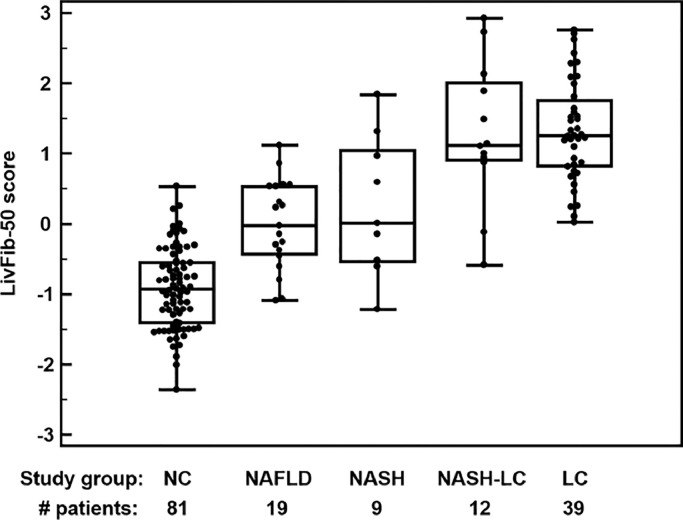
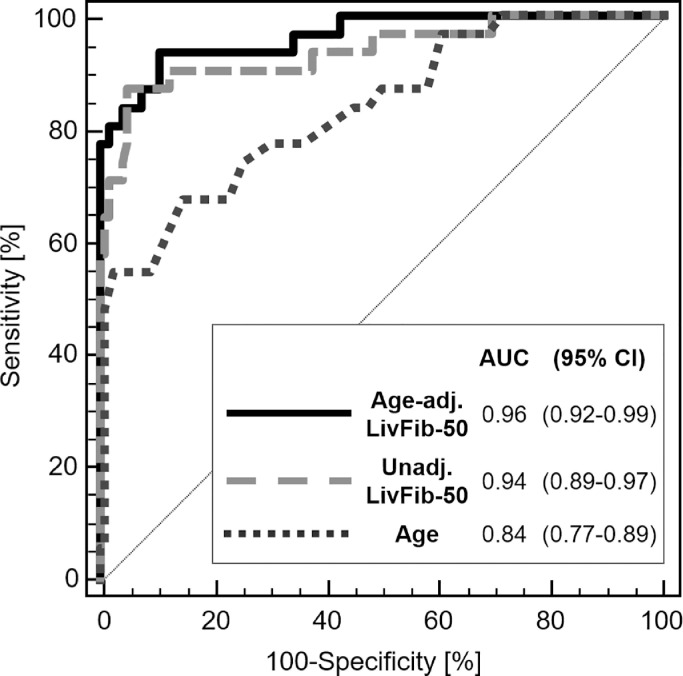
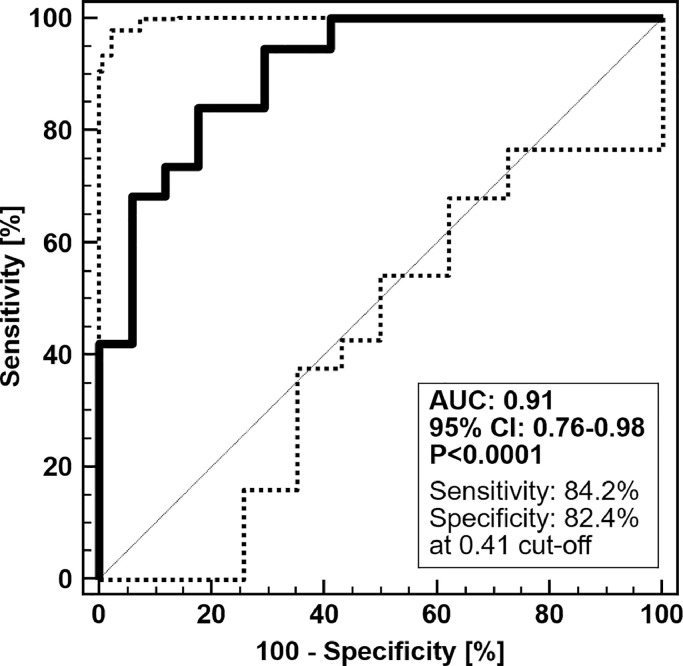
Findings: CE-MS enabled identification of 50 urinary peptides associated with liver fibrosis. When combined into a classifier, LivFib-50, it separated patients with liver fibrosis (N = 31) from non-liver disease controls (N = 123) in cross-sectional diagnostic phase II evaluation with an area under the curve (AUC) of 0.94 (95% confidence intervals (CI): 0.89-0.97, p<0.0001). When adjusted for age, LivFib-50 demonstrated an AUC of 0.94 (95% CI: 0.89-0.97, p<0.0001) in chronic liver disease patients with (N = 19) or without (N = 17) liver fibrosis progression. In this prospective diagnostic phase III validation set, age-adjusted LivFib-50 showed 84.2% sensitivity (95% CI: 60.4-96.6) and 82.4% specificity (95% CI: 56.6-96.2) for detection of liver fibrosis. The sequence-identified peptides are mainly fragments of collagen chains, uromodulin and Na/K-transporting ATPase subunit γ. We also identified ten putative proteolytic cleavage sites, eight were specific for matrix metallopeptidases and two for cathepsins.
Interpretation: In liver fibrosis, urinary peptides profiling offers potential diagnostic markers and leads to discovery of proteolytic sites that could be targets for developing anti-fibrotic therapy.
Keywords: Capillary electrophoresis mass spectrometry; Diagnosis; Liver fibrosis; Urinary peptide marker.
Copyright © 2020 The Author(s). Published by Elsevier B.V. All rights reserved.
Conflict of interest statement
Declaration of Competing Interest Harald Mischak is founder and co-owner of Mosaiques Diagnostics GmbH, which developed the CE-MS technology. Jochen Metzger, Agnieszka Latosinska and Martin Pejchinovski are employees of Mosaiques Diagnostics GmbH. All other authors declare no conflict of interest.
Figures
References
-
- Chalasani N., Younossi Z., Lavine J.E., Diehl A.M., Brunt E.M., Cusi K. The diagnosis and management of non-alcoholic fatty liver disease: practice guideline by the American association for the study of liver diseases, American college of gastroenterology, and the American gastroenterological association. Hepatology. 2012;55:2005–2023. - PubMed
-
- Bedossa P., Patel K. Biopsy and noninvasive methods to assess progression of nonalcoholic fatty liver disease. Gastroenterology. 2016;150 1811-22.e4. - PubMed
-
- Machado M.V., Cortez-Pinto H. Non-invasive diagnosis of non-alcoholic fatty liver disease. A critical appraisal. J Hepatol. 2013;58:1007–1019. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
