

Computed tomography versus magnetic resonance imaging in high-dose-rate prostate brachytherapy planning: The impact on patient-reported health-related quality of life
- PMID: 33160849
- PMCID: PMC8691573
- DOI: 10.1016/j.brachy.2020.09.002
Computed tomography versus magnetic resonance imaging in high-dose-rate prostate brachytherapy planning: The impact on patient-reported health-related quality of life
Abstract
Purpose: High-dose-rate (HDR) prostate brachytherapy uses volumetric imaging for treatment planning. Our institution transitioned from computed tomography (CT)-based planning to MRI-based planning with the hypothesis that improved visualization could reduce treatment-related toxicity. This study aimed to compare the patient-reported health-related quality of life (hrQOL) and physician-graded toxicity outcomes of CT-based and MRI-based HDR prostate brachytherapy.
Methods: From 2016 to 2019, 122 patients with low- or intermediate-risk prostate cancer were treated with HDR brachytherapy as monotherapy. Patients underwent CT only or CT and MRI imaging for treatment planning and were grouped per treatment planning imaging modality. Patient-reported hrQOL in the genitourinary (GU), gastrointestinal (GI), and sexual domains was assessed using International Prostate Symptom Score and Expanded Prostate Cancer Index Composite Short Form-26 questionnaires. Baseline characteristics, changes in hrQOL scores, and physician-graded toxicities were compared between groups.
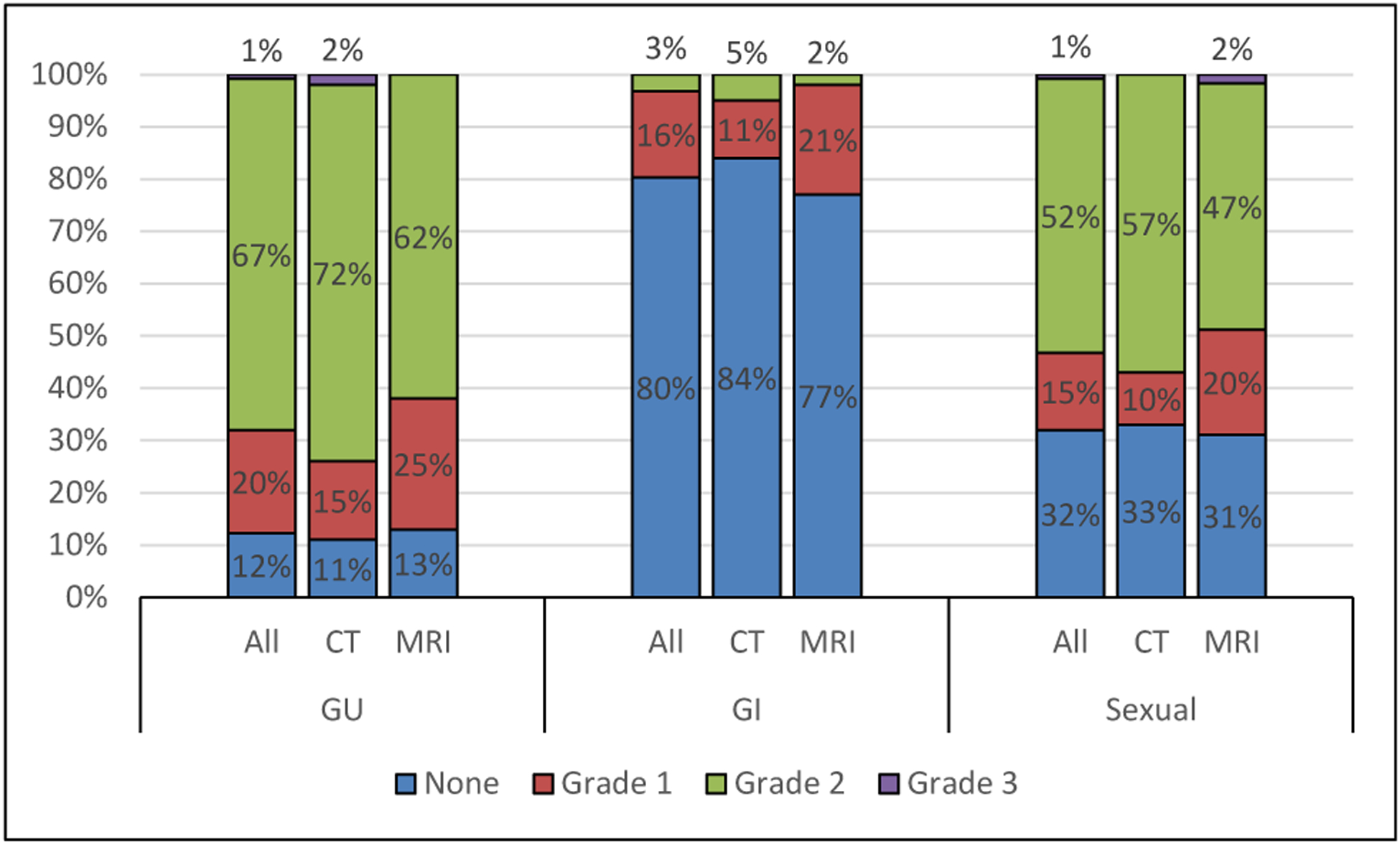
Results: The median follow-up was 18 months. Patient-reported GU, GI, and sexual scores worsened after treatment but returned toward baseline over time. The CT cohort had a lower baseline mean International Prostate Symptom Score (5.8 vs. 7.8, p = 0.03). The other patient-reported GU and GI scores did not differ between groups. Overall, sexual scores were similar between the CT and MRI cohorts (p = 0.08) but favored the MRI cohort at later follow-up with a smaller decrease in Expanded Prostate Cancer Index Composite Short Form-26 sexual score from baseline at 18 months (4.9 vs. 19.8, p = 0.05). Maximum physician-graded GU, GI, and sexual toxicity rates of grade ≥2 were 68%, 3%, and 53%, respectively, with no difference between the cohorts (p = 0.31).
Conclusion: Our study shows that CT- and MRI-based HDR brachytherapy results in similar rates of GU and GI toxicity. MRI-based planning may result in improved erectile function recovery compared with CT-based planning.
Keywords: Computed tomography planning; High-dose-rate brachytherapy; Magnetic resonance imaging planning; Patient-reported toxicity; Prostate cancer; Quality of life.
Published by Elsevier Inc.
Figures


References
-
- Yoshioka Y, Konishi K, Sumida I, et al. Monotherapeutic high-dose-rate brachytherapy for prostate cancer: five-year results of an extreme hypofractionation regimen with 54 GY in nine fractions. Int J Radiat Oncol Biol Phys, 80, 469–475. - PubMed
-
- Yoshioka Y, Konishi K, Oh R, et al. High-dose-rate brachytherapy without external beam irradiation for locally advanced prostate cancer. Radiother Oncol, 80, 62–68. - PubMed
-
- Demanes DJ, Martinez AA, Ghilezan M, et al. High-dose-rate monotherapy: safe and effective brachytherapy for patients with localized prostate cancer. Int J Radiat Oncol Biol Phys 2011;81: 1286–1292. - PubMed
-
- Hoskin P, Rojas A, Ostler P, et al. High-dose-rate brachytherapy with two or three fractions as monotherapy in the treatment of locally advanced prostate cancer. Radiother Oncol 2014;112:63–67. - PubMed
-
- Strouthos I, Tselis N, Chatzikonstantinou G, et al. High dose rate brachytherapy as monotherapy for localised prostate cancer. Radiother Oncol 2018;126:270–277. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
