

Computed tomography-adjusted fistula risk score for predicting clinically relevant postoperative pancreatic fistula after pancreatoduodenectomy: Training and external validation of model upgrade
- PMID: 33161232
- PMCID: PMC7648191
- DOI: 10.1016/j.ebiom.2020.103096
Computed tomography-adjusted fistula risk score for predicting clinically relevant postoperative pancreatic fistula after pancreatoduodenectomy: Training and external validation of model upgrade
Abstract
Background: To develop a modified Fistula Risk Score (FRS) for predicting clinically relevant postoperative pancreatic fistula (CR-POPF) after pancreatoduodenectomy (PD) based on both FRS and contrast-enhanced computed tomography (CE-CT).
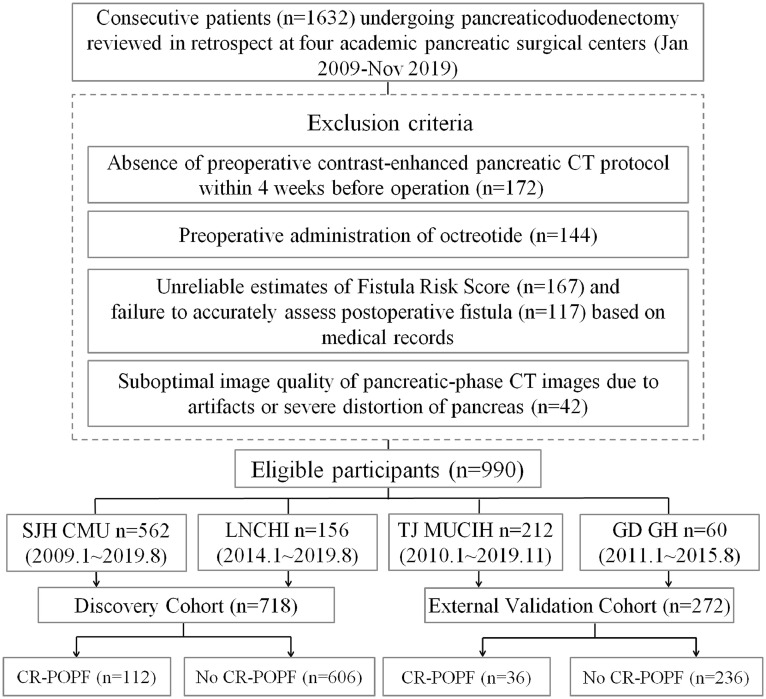
Methods: In this multicenter retrospective analysis, we focused on 990 consecutive patients with pancreatoduodenectomy performed at four institutions between 2009 and 2019. The enhanced CT-FRS model initially targeted 26 pre- and intraoperative factors, including CT descriptors, FRS elements and clinical factors, using LASSO-penalized multivariable logistic regression for predicting CR-POPF events in discovery (n = 718) and externally validated (n = 272) datasets. Probabilities generated were further correlated with histologic features of pancreatic stumps in 356 patients. C-indices were analyzed to compare the predictive potential between the original FRS and the CT-FRS.
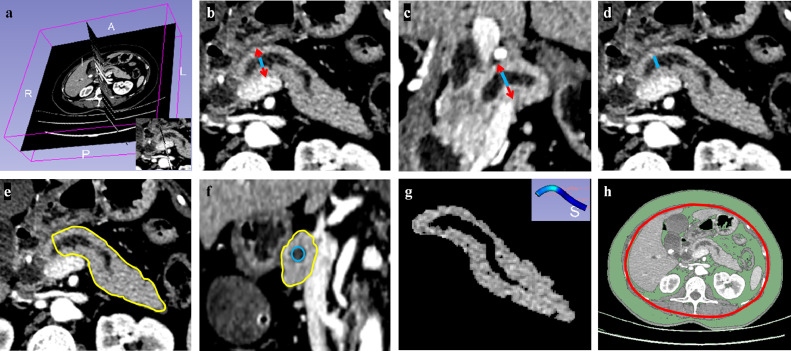
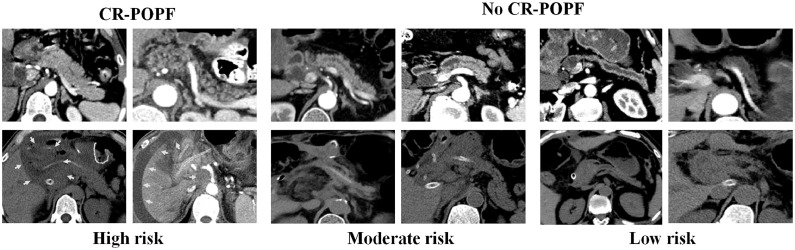
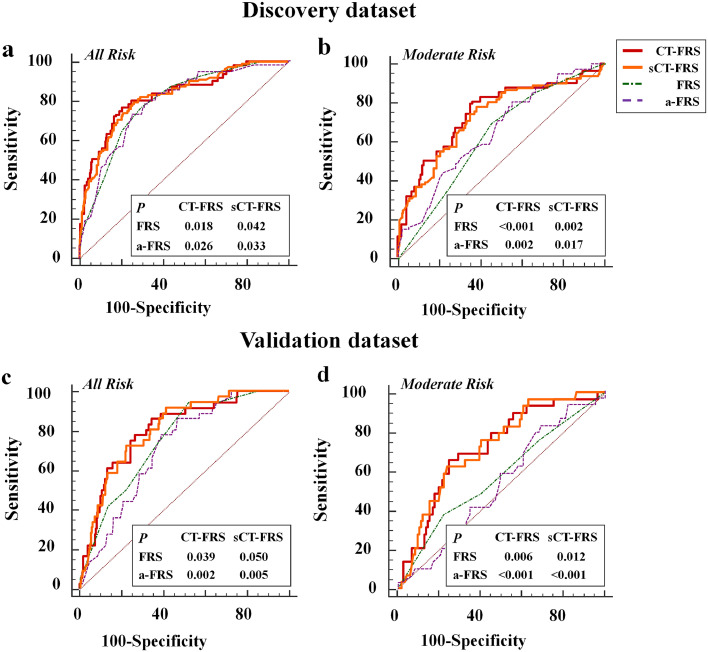
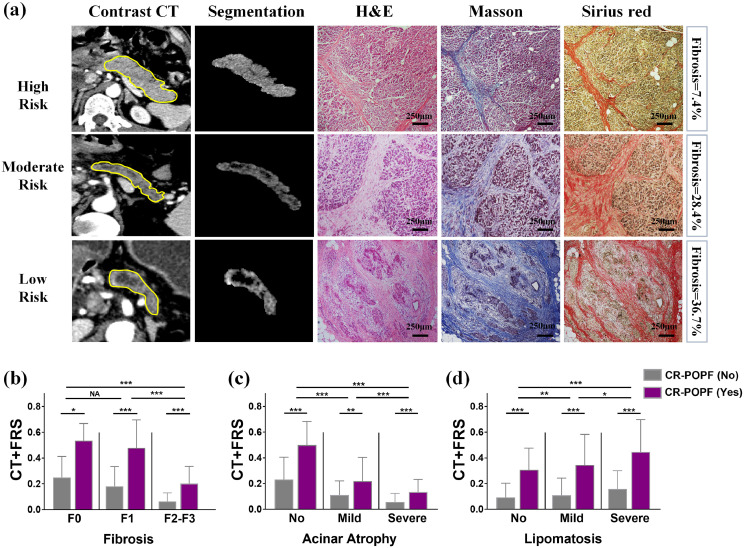
Findings: CR-POPF developed in 112 (15.6%) and 36 (13.2%) patients in discovery and validation datasets, respectively. The final CT-FRS construct, incorporating remnant pancreatic volume (RPV), stump area, fat and atrophy scores by CT, and main pancreatic duct size, offered significantly greater overall predictability than the original FRS in discovery (C-index: 0.825 vs 0.794; p = 0.04) and validation (0.807 vs 0.741; p = 0.05) cohorts. Importantly, it outperformed the FRS in patients at moderate risk levels (FRS: 3-6), showing remarkably improved C-indices (discovery: 0.729 vs 0.626 [p<0.001], validation: 0.722 vs 0.573 [p = 0.006]). CT-FRS probabilities increased in conjunction with less extensive pancreatic fibrosis (p<0.001), ample glandular acini (p<0.001), and advanced lipomatosis (p<0.001).
Interpretation: The enhanced CT-FRS performed significantly better than the original FRS in predicting CR-POPF occurrences after PD, especially at moderate FRS levels.
Keywords: Computed tomography; Pancreaticoduodenectomy; Postoperative pancreatic fistula; Risk prediction.
Copyright © 2020 The Authors. Published by Elsevier B.V. All rights reserved.
Conflict of interest statement
Declaration of Competing Interest None of the authors has any conflict of interest to declare. Yu Shi and Feng Gao contributed equally to this manuscript as the co-first authors.
Figures
References
-
- Nakeeb A., Lillemoe K.D., Cameron J.L. The role of pancreaticoduodenectomy for locally recurrent or metastatic carcinoma to the periampullary region. J Am Coll Surg. 1995;180(2):188–192. - PubMed
-
- Büchler M.W., Wagner M., Schmied B.M., Uhl W., Friess H., Z'graggen K. Changes in morbidity after pancreatic resection: toward the end of completion pancreatectomy. Arch Surg. 2003;138(12):1310–1314. - PubMed
-
- Poon R.T.P., Lo S.H., Fong D., Fan S.T., Wong J. Prevention of pancreatic anastomotic leakage after pancreaticoduodenectomy. Am J Surg. 2002;183(1):42–52. - PubMed
