

Premature Menopause, Clonal Hematopoiesis, and Coronary Artery Disease in Postmenopausal Women
- PMID: 33161765
- PMCID: PMC7911856
- DOI: 10.1161/CIRCULATIONAHA.120.051775
Premature Menopause, Clonal Hematopoiesis, and Coronary Artery Disease in Postmenopausal Women
Abstract
Background: Premature menopause is an independent risk factor for cardiovascular disease in women, but mechanisms underlying this association remain unclear. Clonal hematopoiesis of indeterminate potential (CHIP), the age-related expansion of hematopoietic cells with leukemogenic mutations without detectable malignancy, is associated with accelerated atherosclerosis. Whether premature menopause is associated with CHIP is unknown.
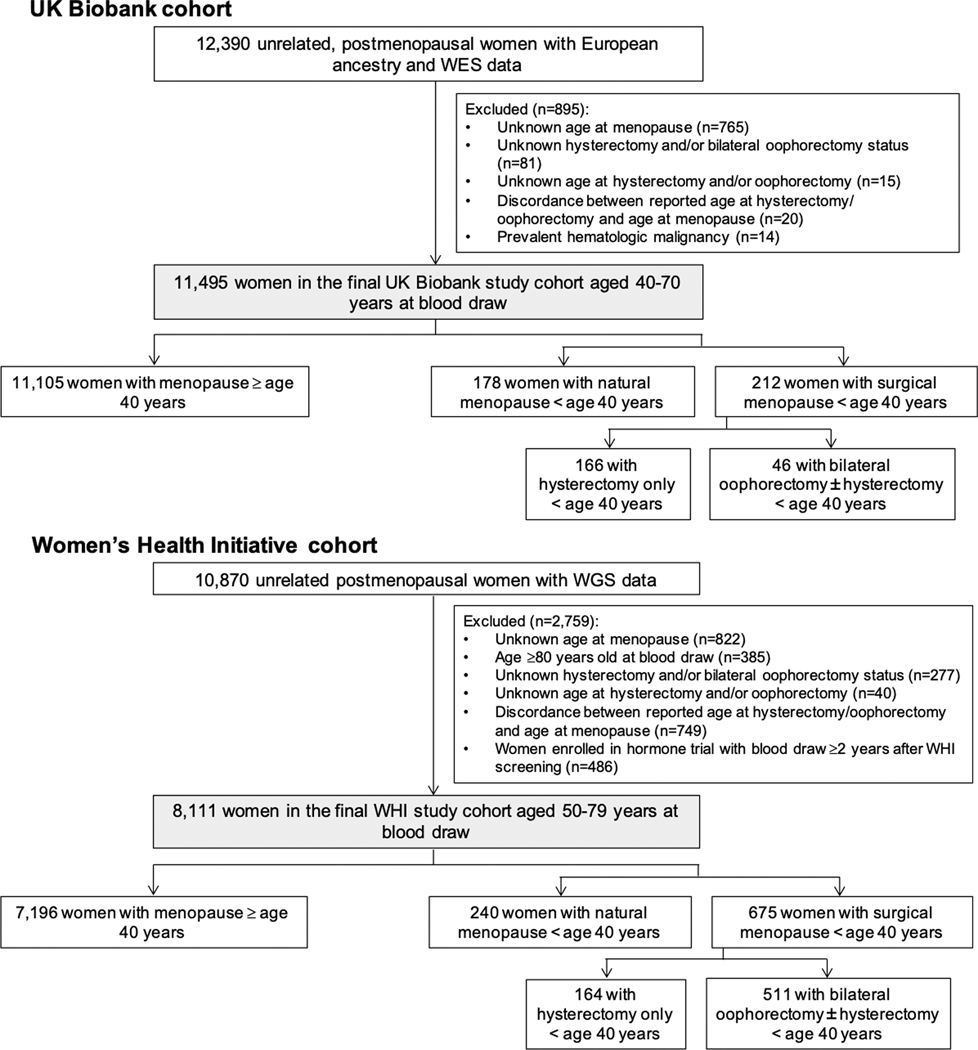
Methods: We included postmenopausal women from the UK Biobank (n=11 495) aged 40 to 70 years with whole exome sequences and from the Women's Health Initiative (n=8111) aged 50 to 79 years with whole genome sequences. Premature menopause was defined as natural or surgical menopause occurring before age 40 years. Co-primary outcomes were the presence of any CHIP and CHIP with variant allele frequency >0.1. Logistic regression tested the association of premature menopause with CHIP, adjusted for age, race, the first 10 principal components of ancestry, smoking, diabetes, and hormone therapy use. Secondary analyses considered natural versus surgical premature menopause and gene-specific CHIP subtypes. Multivariable-adjusted Cox models tested the association between CHIP and incident coronary artery disease.
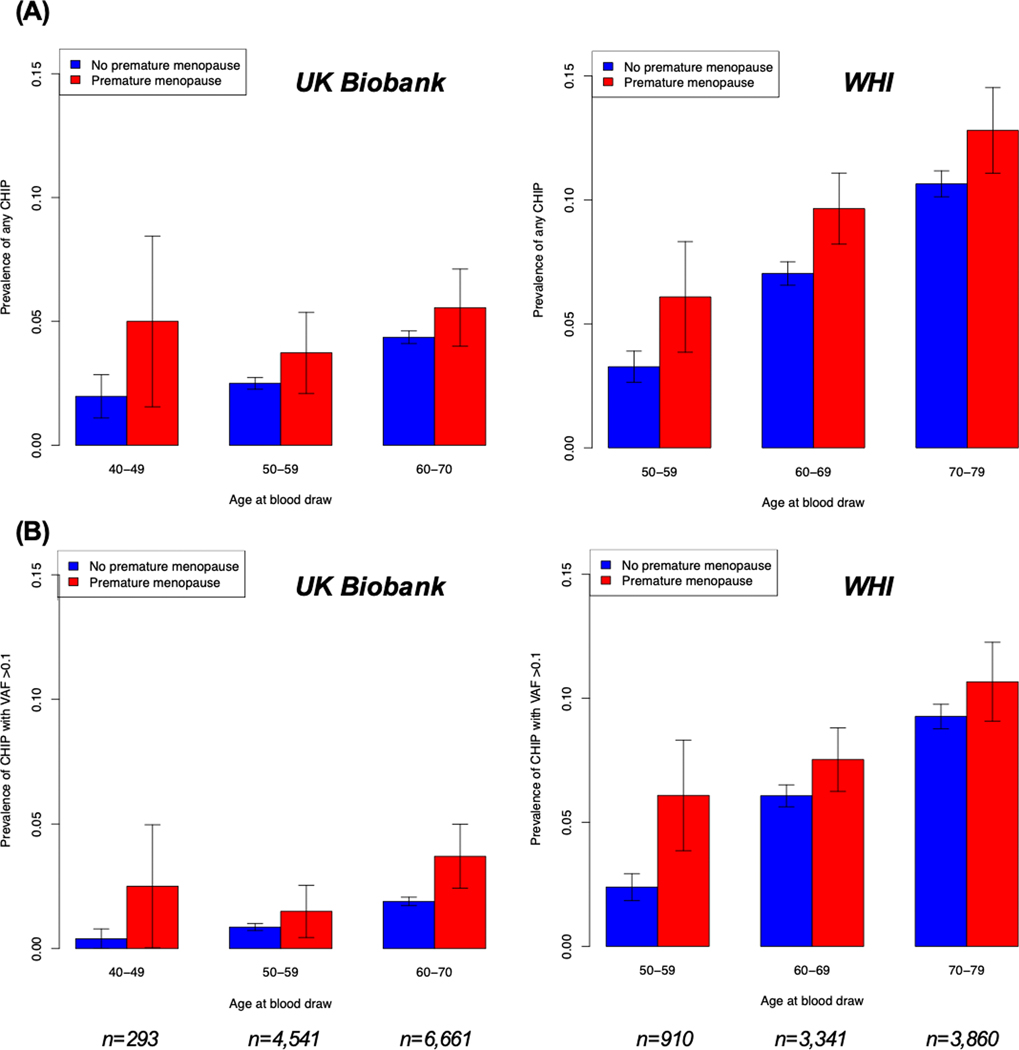
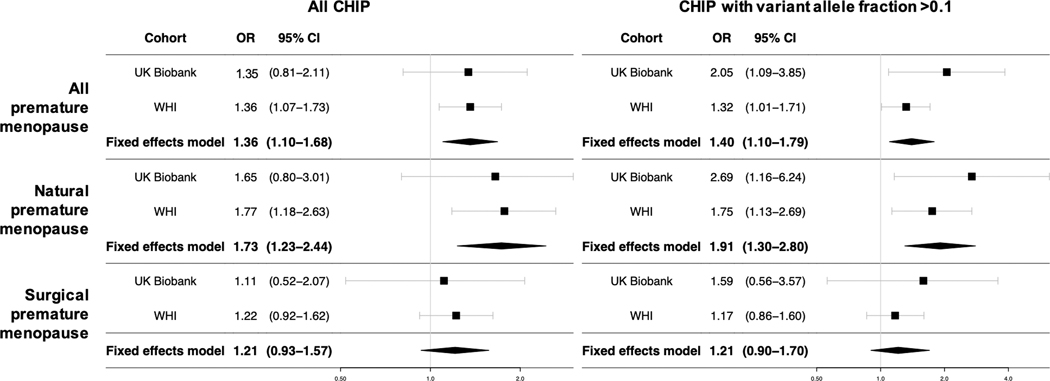
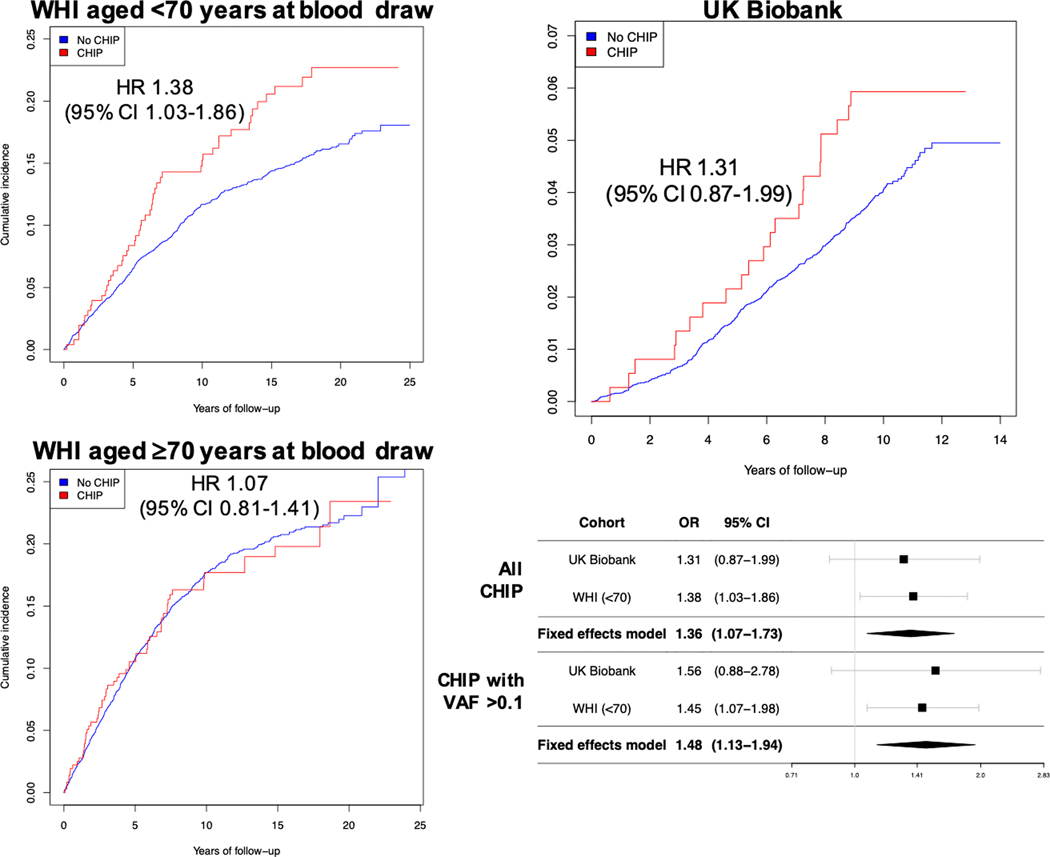
Results: The sample included 19 606 women, including 418 (2.1%) with natural premature menopause and 887 (4.5%) with surgical premature menopause. Across cohorts, CHIP prevalence in postmenopausal women with versus without a history of premature menopause was 8.8% versus 5.5% (P<0.001), respectively. After multivariable adjustment, premature menopause was independently associated with CHIP (all CHIP: odds ratio, 1.36 [95% 1.10-1.68]; P=0.004; CHIP with variant allele frequency >0.1: odds ratio, 1.40 [95% CI, 1.10-1.79]; P=0.007). Associations were larger for natural premature menopause (all CHIP: odds ratio, 1.73 [95% CI, 1.23-2.44]; P=0.001; CHIP with variant allele frequency >0.1: odds ratio, 1.91 [95% CI, 1.30-2.80]; P<0.001) but smaller and nonsignificant for surgical premature menopause. In gene-specific analyses, only DNMT3A CHIP was significantly associated with premature menopause. Among postmenopausal middle-aged women, CHIP was independently associated with incident coronary artery disease (hazard ratio associated with all CHIP: 1.36 [95% CI, 1.07-1.73]; P=0.012; hazard ratio associated with CHIP with variant allele frequency >0.1: 1.48 [95% CI, 1.13-1.94]; P=0.005).
Conclusions: Premature menopause, especially natural premature menopause, is independently associated with CHIP among postmenopausal women. Natural premature menopause may serve as a risk signal for predilection to develop CHIP and CHIP-associated cardiovascular disease.
Keywords: clonal hematopoiesis; coronary artery disease; hematology; inflammation; menopause, premature; women.
Conflict of interest statement
The other authors declare no competing interests.
Figures
Comment in
-
Clonal Hematopoiesis and Premature Menopause: Unexpected Liaison.Circulation. 2021 Feb 2;143(5):424-426. doi: 10.1161/CIRCULATIONAHA.120.052293. Epub 2021 Feb 1. Circulation. 2021. PMID: 33523729 No abstract available.
References
-
- Virani SS, Alonso A, Benjamin EJ, Bittencourt MS, Callaway CW, Carson AP, Chamberlain AM, Chang AR, Cheng S, Delling FN, et al. Heart Disease and Stroke Statistics-2020 Update: A Report From the American Heart Association. Circulation. 2020;141:e139–e596. doi: 10.1161/CIR.0000000000000757 - DOI - PubMed
Publication types
MeSH terms
Grants and funding
- T32 HL094301/HL/NHLBI NIH HHS/United States
- HHSN268201600002C/HL/NHLBI NIH HHS/United States
- R01 HL151283/HL/NHLBI NIH HHS/United States
- HHSN268201600018C/HL/NHLBI NIH HHS/United States
- R01 HL134892/HL/NHLBI NIH HHS/United States
- R01 HL142711/HL/NHLBI NIH HHS/United States
- HHSN268201800001C/HL/NHLBI NIH HHS/United States
- HHSN268201600003C/HL/NHLBI NIH HHS/United States
- HHSN268201600004C/HL/NHLBI NIH HHS/United States
- MC_PC_17228/MRC_/Medical Research Council/United Kingdom
- R01 HL117626/HL/NHLBI NIH HHS/United States
- R01 HL148050/HL/NHLBI NIH HHS/United States
- DP5 OD029586/OD/NIH HHS/United States
- R01 HL120393/HL/NHLBI NIH HHS/United States
- MC_QA137853/MRC_/Medical Research Council/United Kingdom
- P30 ES006694/ES/NIEHS NIH HHS/United States
- U01 HL120393/HL/NHLBI NIH HHS/United States
- R01 HL148565/HL/NHLBI NIH HHS/United States
- HHSN268201500014C/HL/NHLBI NIH HHS/United States
- HHSN268201600001C/HL/NHLBI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
