

Surgical Treatment for Crohn's Disease: A Role of Kono-S Anastomosis in the West
- PMID: 33162837
- PMCID: PMC7605911
- DOI: 10.1055/s-0040-1714236
Surgical Treatment for Crohn's Disease: A Role of Kono-S Anastomosis in the West
Abstract
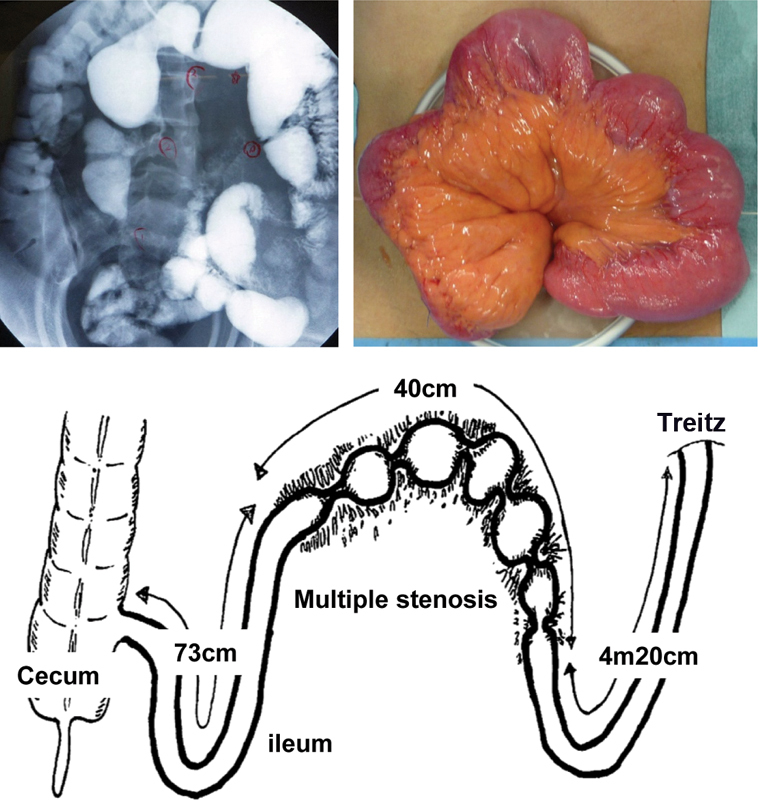
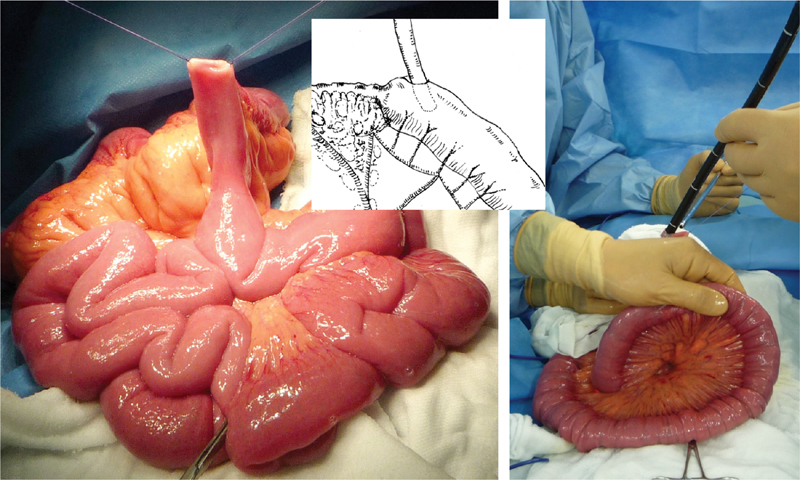
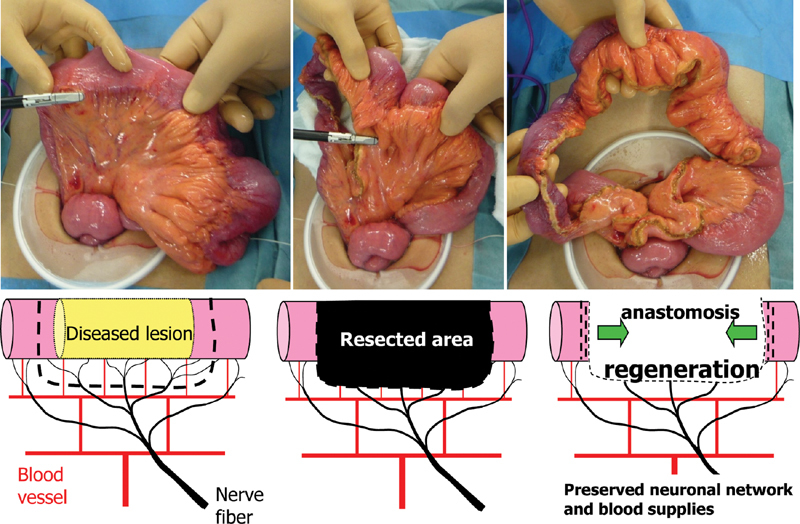
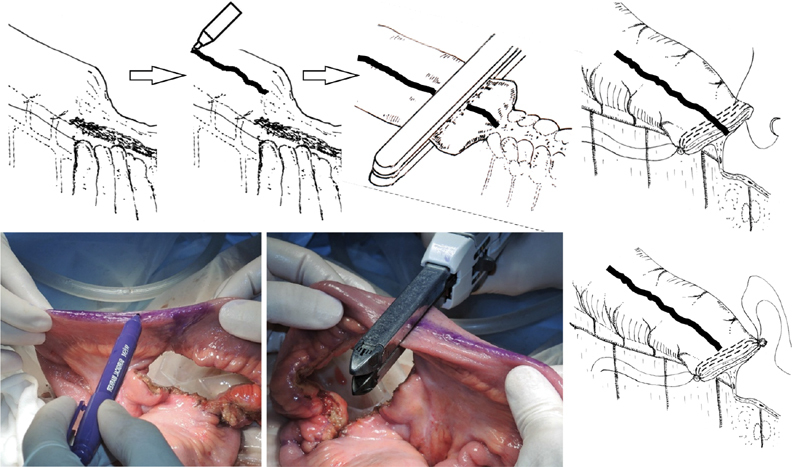
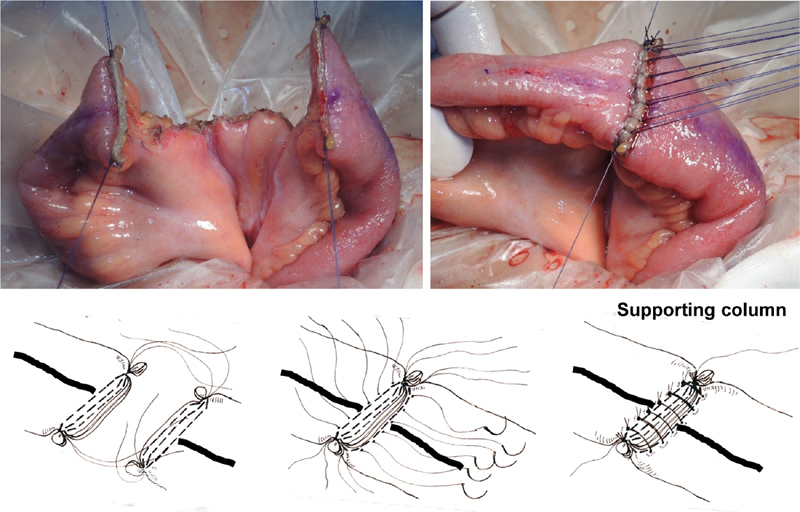
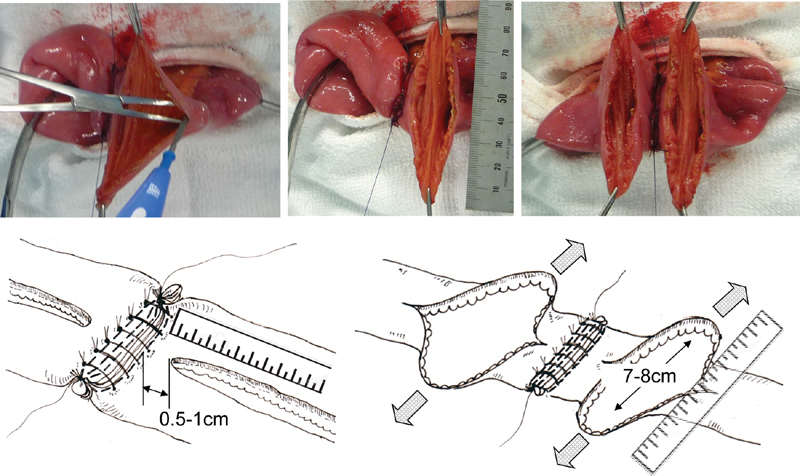
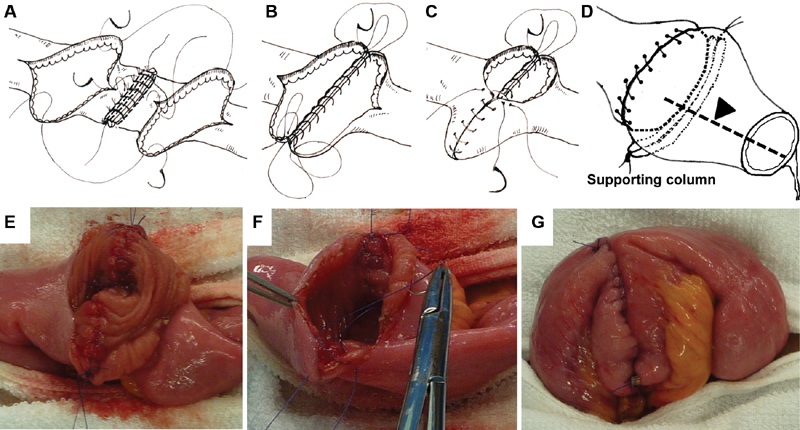
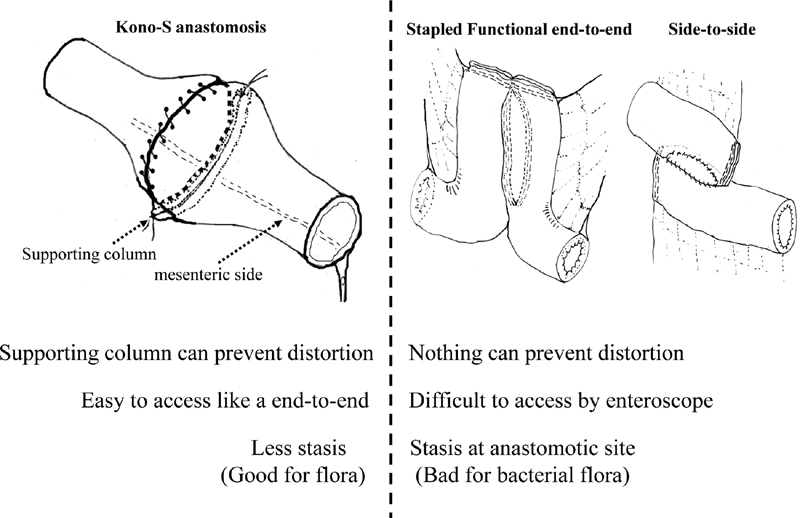
More than 80% of patients with Crohn's disease (CD) will require surgical intervention during their lifetime, with high rates of anastomotic recurrence and stenosis necessitating repeat surgery. Current data show that pharmacotherapy has not significantly improved the natural history of postoperative clinical and surgical recurrence of CD. In 2003, antimesenteric hand-sewn functional end-to-end (Kono-S) anastomosis was first performed in Japan. This technique has yielded very desirable outcomes in terms of reducing the incidence of anastomotic surgical recurrence. The most recent follow-up of these patients showed that very few had developed surgical recurrence. This new approach is superior to stapled functional end-to-end anastomosis because the stumps are sutured together to create a stabilizing structure (a "supporting column"), serving as a supportive backbone of the anastomosis to help prevent distortion of the anastomotic lumen due to disease recurrence and subsequent clinical symptoms. This technique requires careful mesenteric excision for optimal preservation of the blood supply and innervation. It also results in a very wide anastomotic lumen on the antimesenteric side. The Kono-S technique has shown efficacy in preventing surgical recurrence and the potential to become the new standard of care for intestinal CD.
Keywords: Crohn’s disease; stapled functional end-to-end anastomosis; supporting column; surgical recurrence.
© Thieme Medical Publishers.
Conflict of interest statement
Conflict of Interest None.
Figures
References
-
- Baumgart D C, Sandborn W J.Crohn's disease Lancet 2012380(9853):1590–1605. - PubMed
-
- Fichera A, Schlottmann F, Krane M, Bernier G, Lange E. Role of surgery in the management of Crohn's disease. Curr Probl Surg. 2018;55(05):162–187. - PubMed
-
- Terdiman J P. Prevention of postoperative recurrence in Crohn's disease. Clin Gastroenterol Hepatol. 2008;6(06):616–620. - PubMed
