

Assessment of three-dimensional acetabular coverage angles
- PMID: 33163216
- PMCID: PMC7605764
- DOI: 10.1093/jhps/hnaa026
Assessment of three-dimensional acetabular coverage angles
Abstract
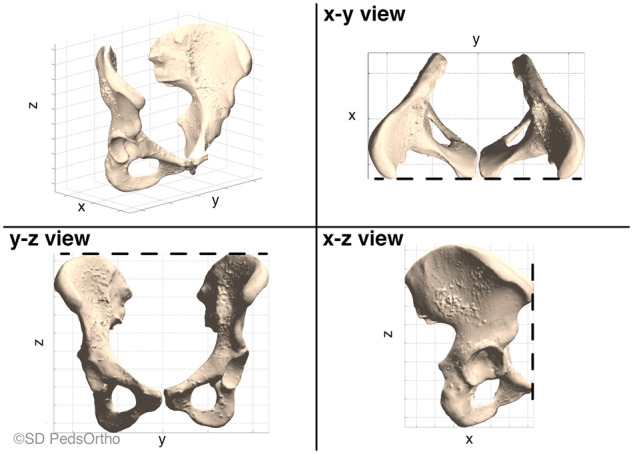
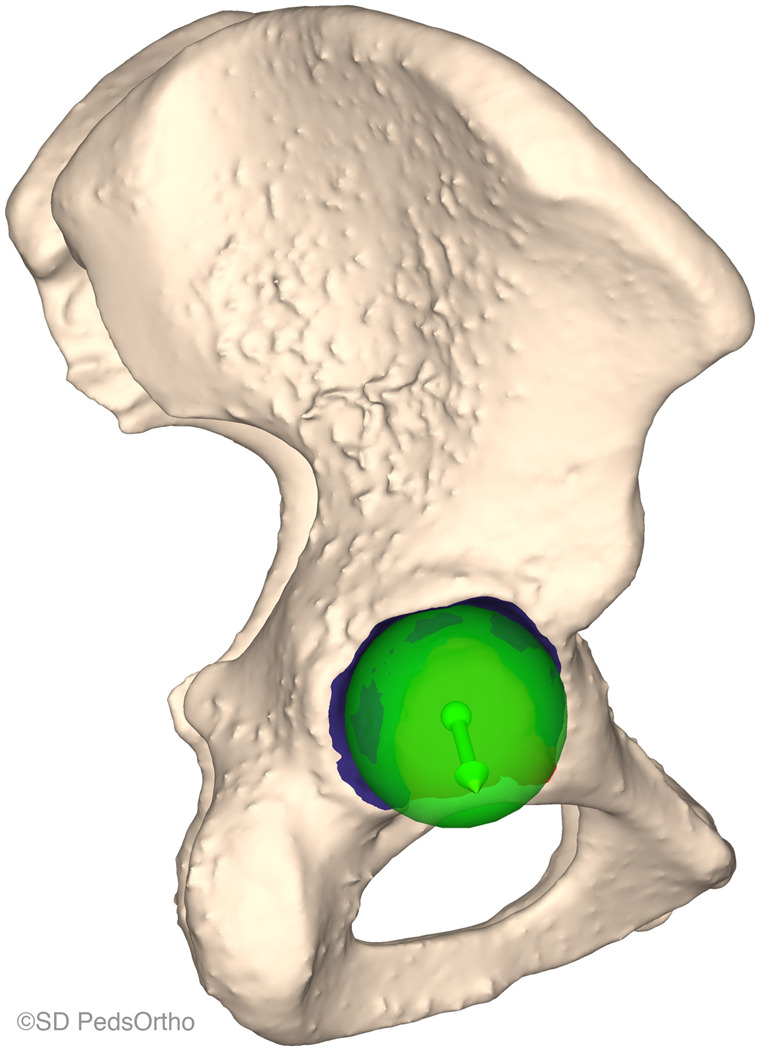
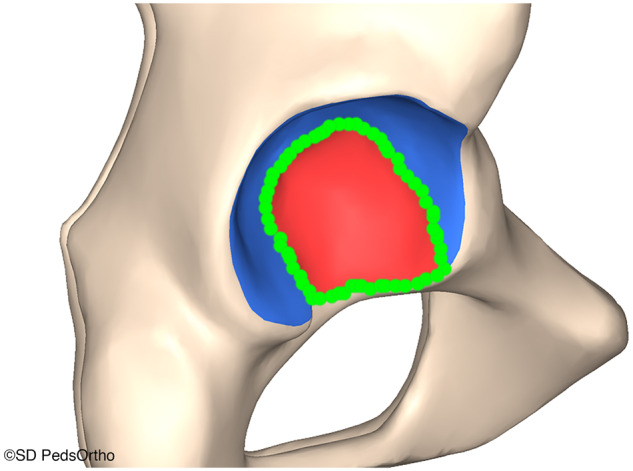
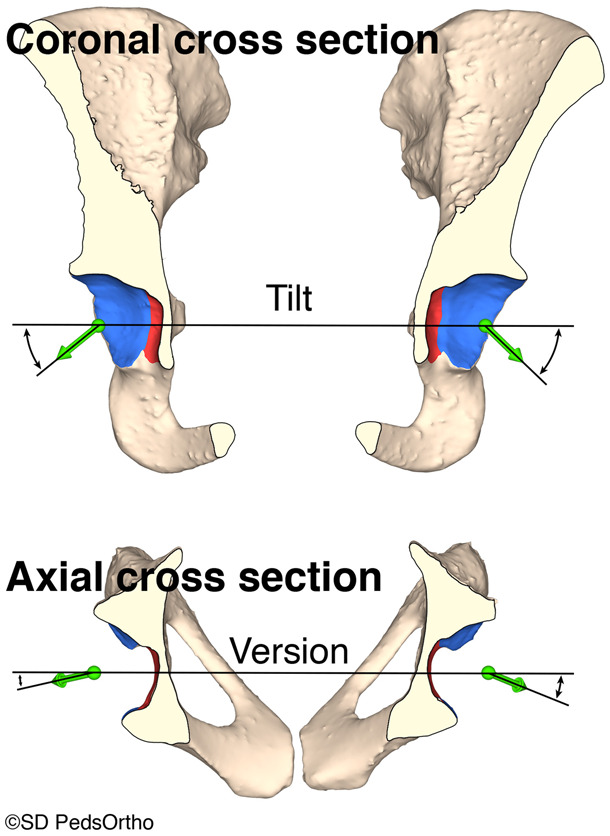
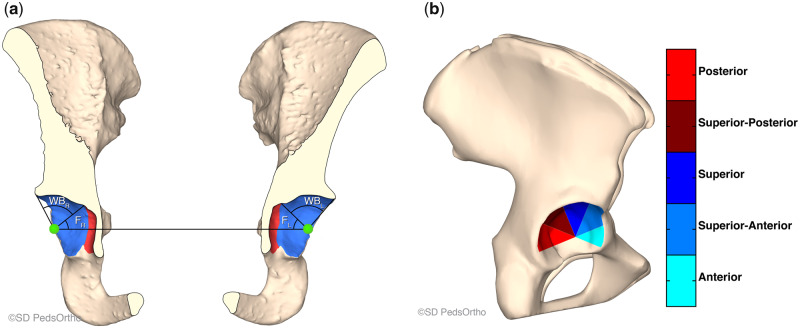
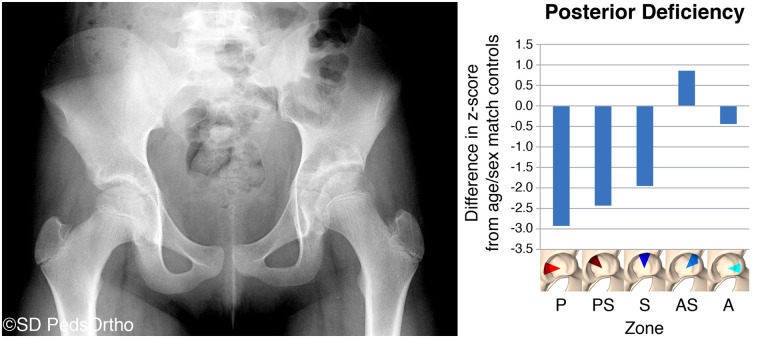
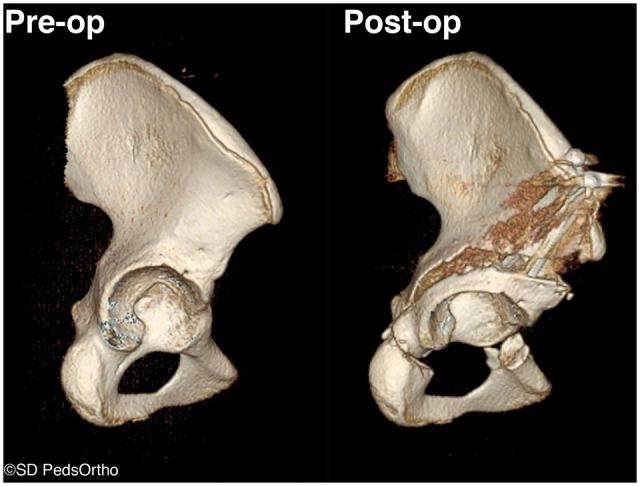
The purpose of this article is to report the inter- and intra-observer reliability of a computerized objective technique to quantify patient-specific acetabular morphology. We describe the use of and provide the software code for a technique to better define the location and magnitude of acetabular pathology. We have developed software code that allows the end user to obtain detailed measurements of the acetabulum using traditional computed tomography data. We provide the code and detailed instructions on how to use it in this article. The methodology was validated by having an unbiased observer (that was not involved in this project but has been trained in this software measurement methodology) to perform the entire acquisition, reconstruction and analysis procedure and compare their measurements to the measurements of one of the authors. The author then repeated the procedure 2 months later to determine intra-observer reliability. Inter- and intra-observer reliability for version, tilt, surface area and total acetabular coverage angles ranged from an intra-class correlation coefficient of 0.805 to 0.997. The method provided in this manuscript gives a reproducible objective assessment of three-dimensional (3D) acetabular morphology that can be used to assist in the diagnosis of hip pathology and to compare the morphological parameters of subjects with and without hip pathology. It allows a surgeon to understand the 3D shape of each individual's acetabulum, share these findings with patients and their parents to demonstrate the magnitude and location of the clinical abnormality and perform patient-specific surgical corrections to optimize the shape and coverage of the hip.
© The Author(s) 2020. Published by Oxford University Press.
Figures
References
-
- Parvaresh KC, Pennock AT, Bomar JD et al. Analysis of acetabular ossification from the triradiate cartilage and secondary centers. J Pediatr Orthop 2018; 38: e145–50. - PubMed
-
- Tönnis D. Congenital Dysplasia and Dislocation of the Hip in Children and Adults. Berlin, Heidelberg: Springer-Verlag, 1987.
