

Understanding Mesangial Pathobiology in AL-Amyloidosis and Monoclonal Ig Light Chain Deposition Disease
- PMID: 33163710
- PMCID: PMC7609979
- DOI: 10.1016/j.ekir.2020.07.013
Understanding Mesangial Pathobiology in AL-Amyloidosis and Monoclonal Ig Light Chain Deposition Disease
Abstract
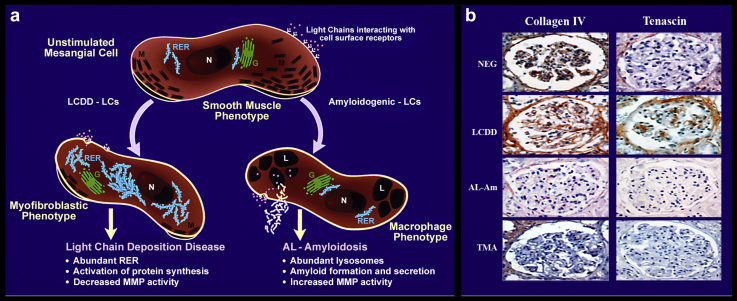
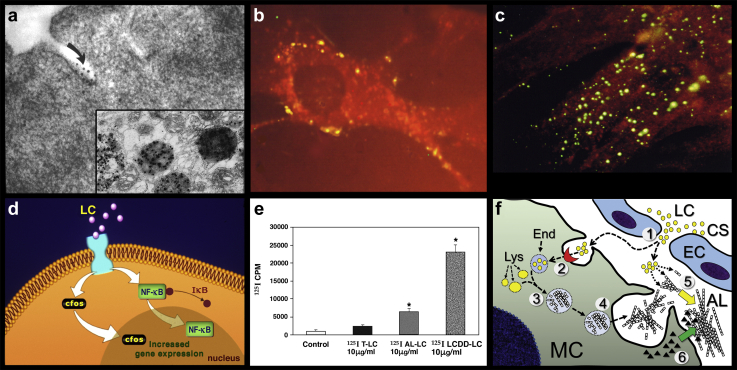
Patients with plasma cell dyscrasias produce free abnormal monoclonal Ig light chains that circulate in the blood stream. Some of them, termed glomerulopathic light chains, interact with the mesangial cells and trigger, in a manner dependent of their structural and physicochemical properties, a sequence of pathological events that results in either light chain-derived (AL) amyloidosis (AL-Am) or light chain deposition disease (LCDD). The mesangial cells play a key role in the pathogenesis of both diseases. The interaction with the pathogenic light chain elicits specific cellular processes, which include apoptosis, phenotype transformation, and secretion of extracellular matrix components and metalloproteinases. Monoclonal light chains associated with AL-Am but not those producing LCDD are avidly endocytosed by mesangial cells and delivered to the mature lysosomal compartment where amyloid fibrils are formed. Light chains from patients with LCDD exert their pathogenic signaling effect at the cell surface of mesangial cells. These events are generic mesangial responses to a variety of adverse stimuli, and they are similar to those characterizing other more frequent glomerulopathies responsible for many cases of end-stage renal disease. The pathophysiologic events that have been elucidated allow to propose future therapeutic approaches aimed at preventing, stopping, ameliorating, or reversing the adverse effects resulting from the interactions between glomerulopathic light chains and mesangium.
Keywords: AL-amyloidosis; kidney; kidney repair; light chain deposition disease; mesangium; monoclonal Ig deposition disease; monoclonal light chains; stem cells.
© 2020 International Society of Nephrology. Published by Elsevier Inc.
Figures
References
-
- Martin T., Huff C.A. Multiple myeloma: current advances and future directions. Clin Lymphoma Myeloma Leuk. 2019;19:255–263. - PubMed
-
- Sanders P.W., Herrera G.A. Monoclonal immunoglobulin light chain-related renal diseases. Semin Nephrol. 1993;13:324–341. - PubMed
-
- Leung N., Bridoux F., Hutchison C.A. Monoclonal gammopathy of renal significance:when MGUS is no longer undetermined or insignificant. Blood. 2012;120:4292–4295. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
