

Rule Out Acute Kidney Injury in the Emergency Department With a Urinary Dipstick
- PMID: 33163719
- PMCID: PMC7609964
- DOI: 10.1016/j.ekir.2020.09.006
Rule Out Acute Kidney Injury in the Emergency Department With a Urinary Dipstick
Abstract
Introduction: The identification of acute injury of the kidney relies on serum creatinine (SCr), a functional marker with poor temporal resolution as well as limited sensitivity and specificity for cellular injury. In contrast, urinary biomarkers of kidney injury have the potential to detect cellular stress and damage in real time.
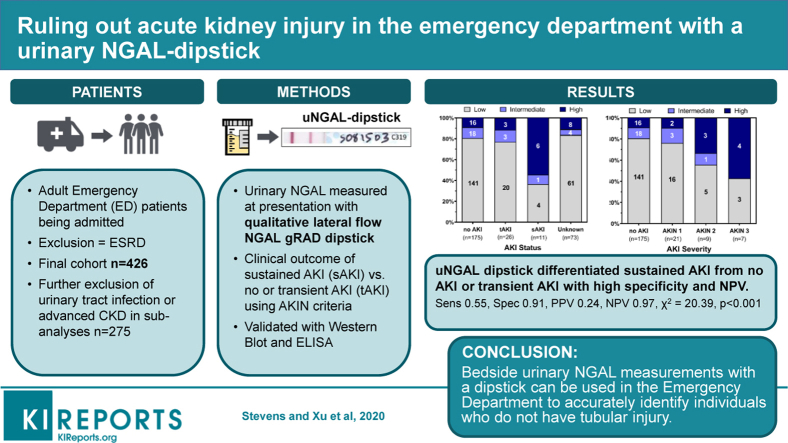
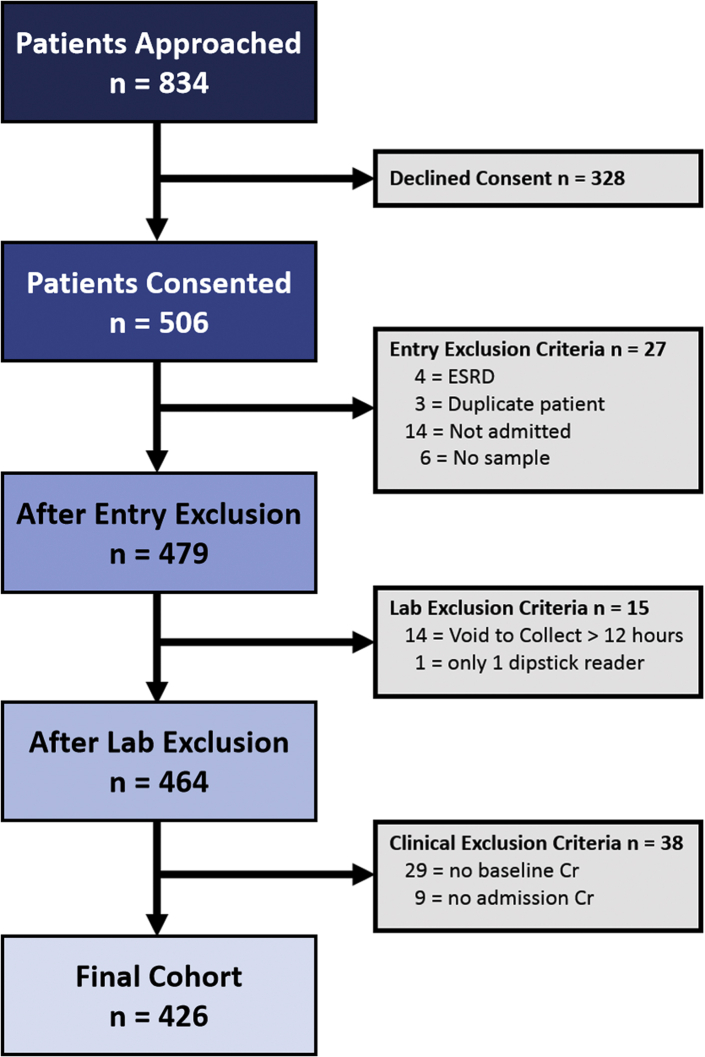
Methods: To detect the response of the kidney to injury, we have tested a lateral flow dipstick that measures a urinary protein called neutrophil gelatinase-associated lipocalin (NGAL). Analysis of urine was performed in a prospective cohort of 479 patients (final cohort N = 426) entering an emergency department in New York City and subsequently admitted for inpatient care.
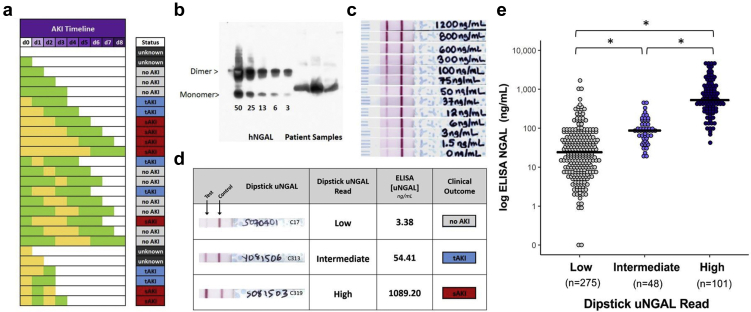
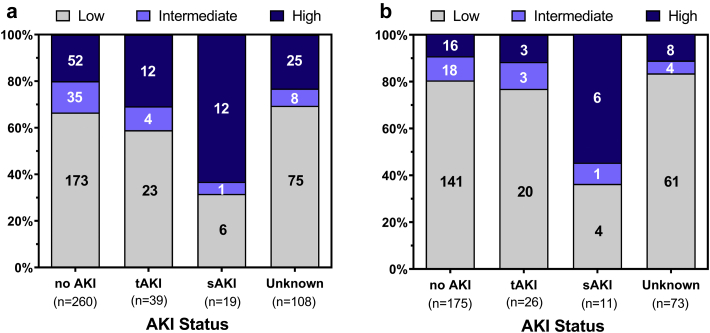
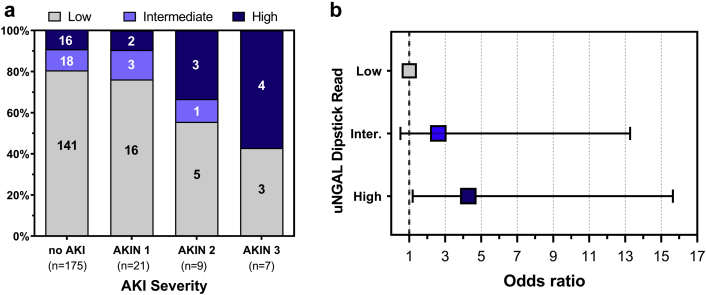
Results: Colorimetric development had high interrater reliability (88% concordance rate) and correlated with traditional enzyme-linked immunosorbent assay (ELISA) measurements (ρ = 0.732, P < .0001). Of the 14% of the cohort who met Acute Kidney Injury Network (AKIN) SCr criteria for acute kidney injury (AKI), 67% demonstrated transient (<2 days) and 33% demonstrated sustained (>2 days) elevation of SCr. Comparing the outcomes of patients with sustained versus transient or undetectable changes in SCr revealed that the urinary NGAL (uNGAL) dipstick had high specificity and negative predictive value (NPV) (high- vs. low-intermediate readings, sensitivity = 0.55, specificity = 0.91, positive predictive value = 0.24, NPV = 0.97, χ2 = 20.39, P < 0.001).
Conclusion: We show that the introduction of a bedside uNGAL dipstick permits accurate triage by identifying individuals who do not have tubular injury. In an era of shortening length of stay and rapid decisions based on isolated SCr measurements, real-time exclusion of kidney injury by a dipstick will be particularly useful to overcome the retrospective, insensitive, and nonspecific attributes of SCr.
Keywords: AKI; NGAL; biomarker; dipstick; emergency department.
© 2020 International Society of Nephrology. Published by Elsevier Inc.
Figures
References
-
- Sharma A., Mucino M.J., Ronco C. Renal functional reserve and renal recovery after acute kidney injury. Nephron Clin Pract. 2014;127:94–100. - PubMed
-
- Vanmassenhove J., Van Biesen W., Vanholder R. Subclinical AKI: ready for primetime in clinical practice? J Nephrol. 2019;32:9–16. - PubMed
-
- Haase M., Kellum J.A., Ronco C. Subclinical AKI--an emerging syndrome with important consequences. Nat Rev Nephrol. 2012;8:735–739. - PubMed
-
- Moretti C., Frajese G.V., Guccione L. Androgens and body composition in the aging male. J Endocrinol Invest. 2005;28:56–64. - PubMed
-
- Kimmel P.L., Lew S.Q., Bosch J.P. Nutrition, ageing and GFR: is age-associated decline inevitable? Nephrol Dial Transplant. 1996;11(suppl 9):85–88. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
