

Effect of Renin-Angiotensin System Inhibitors on the Comparative Nephrotoxicity of NSAIDs and Opioids during Hospitalization
- PMID: 33163971
- PMCID: PMC7643868
- DOI: 10.34067/kid.0001432020
Effect of Renin-Angiotensin System Inhibitors on the Comparative Nephrotoxicity of NSAIDs and Opioids during Hospitalization
Abstract
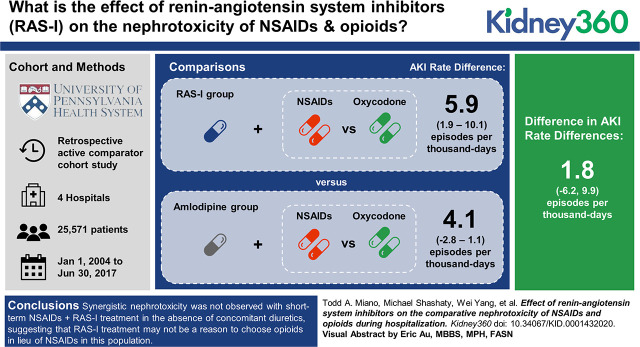
Background: Nonsteroidal anti-inflammatory drugs (NSAIDS) are increasingly important alternatives to opioids for analgesia during hospitalization as health systems implement opioid-minimization initiatives. Increasing NSAID use may increase AKI rates, particularly in patients with predisposing risk factors. Inconclusive data in outpatient populations suggests that NSAID nephrotoxicity is magnified by renin-angiotensin system inhibitors (RAS-I). No studies have tested this in hospitalized patients.
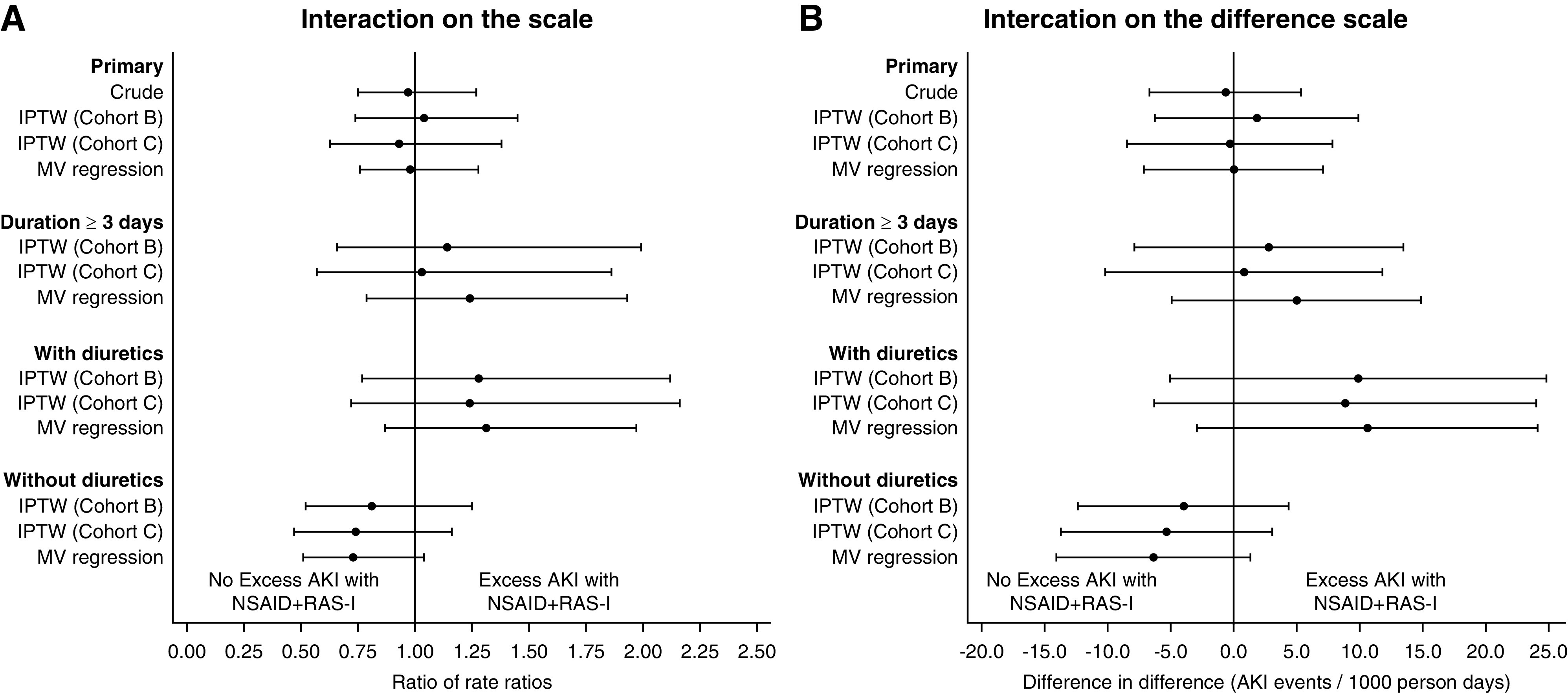
Methods: Retrospective, active-comparator cohort study of patients admitted to four hospitals in Philadelphia, Pennsylvania. To minimize confounding by indication, NSAIDs were compared to oxycodone, and RAS-I were compared to amlodipine. We tested synergistic NSAID+RAS-I nephrotoxicity by comparing the difference in AKI rate between NSAID versus oxycodone in patients treated with RAS-I to the difference in AKI rate between NSAID versus oxycodone in patients treated with amlodipine. In a secondary analysis, we restricted the cohort to patients with baseline diuretic treatment. AKI rates were adjusted for 71 baseline characteristics with inverse probability of treatment-weighted Poisson regression.
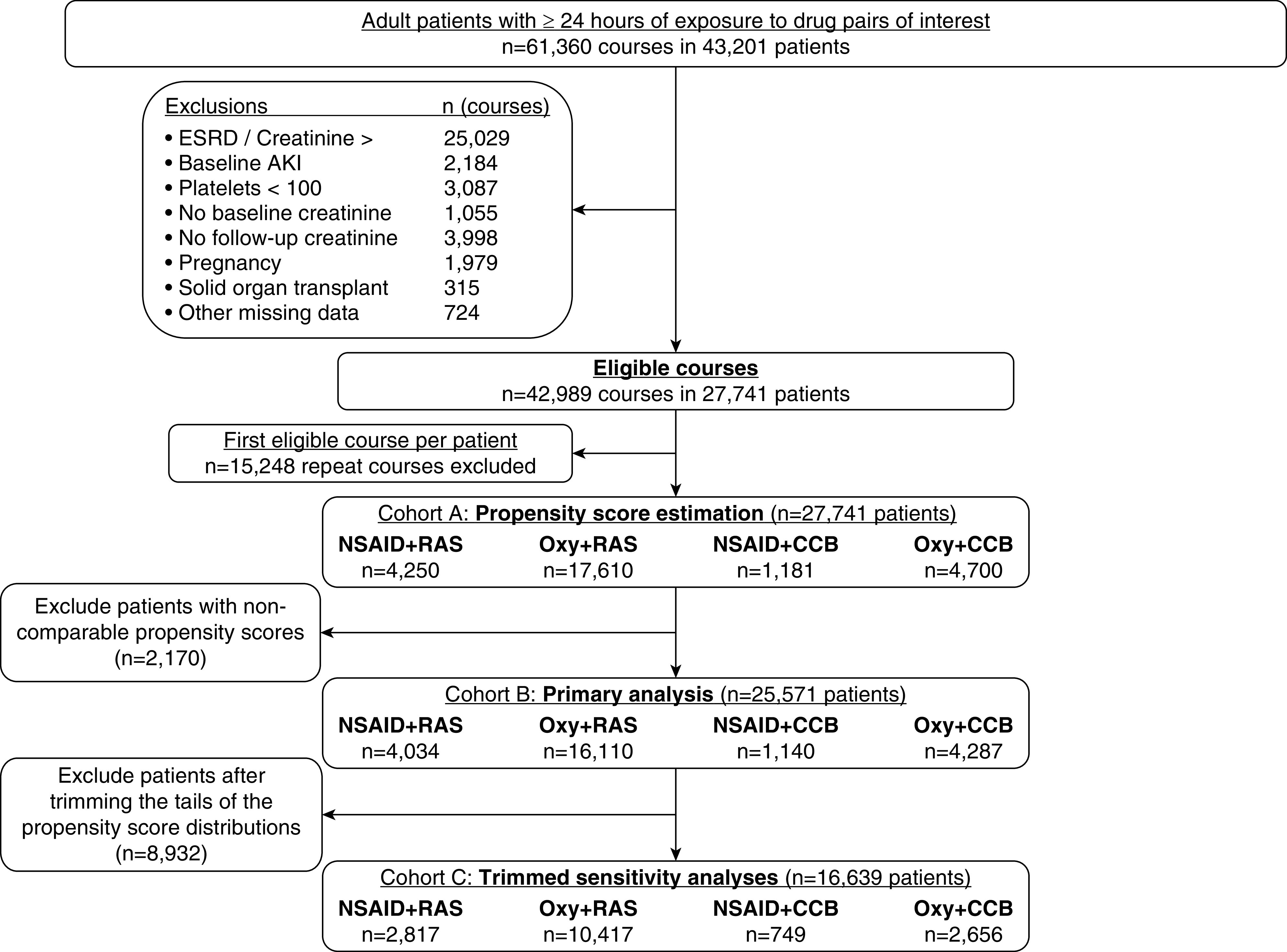
Results: The analysis included 25,571 patients who received a median of 2.4 days of analgesia. The overall AKI rate was 23.6 per 1000 days. The rate difference (RD) for NSAID versus oxycodone in patients treated with amlodipine was 4.1 per 1000 days (95% CI, -2.8 to 11.1), and the rate difference for NSAID versus oxycodone in patients treated with RAS-I was 5.9 per 1000 days (95% CI, 1.9 to 10.1), resulting in a nonsignificant interaction estimate: 1.85 excess AKI events per 1000 days (95% CI, -6.23 to 9.92). Analysis in patients treated with diuretics produced a higher, albeit nonsignificant, interaction estimate: 9.89 excess AKI events per 1000 days (95% CI, -5.04 to 24.83).
Conclusions: Synergistic nephrotoxicity was not observed with short-term NSAID+RAS-I treatment in the absence of concomitant diuretics, suggesting that RAS-I treatment may not be a reason to choose opioids in lieu of NSAIDs in this population. Synergistic nephrotoxicity cannot be ruled out in patients treated with diuretics.
Conflict of interest statement
J. Brown has received consulting fees from Bracco Scientific. S. Hennessy has received consulting fees from the following companies: Braeburn Pharmaceuticals Inc, Esteve Pharmaceuticals LLC, Greenwich Biosciences Inc, Hoffman La Roche, Indivior Inc, Inspiron Delivery Sciences LLC, Janssen Research & Development LLC, Laboratoire HRA PHARMA, Lexicon Pharmaceuticals Inc, Lilly USA LLC, Mallincrodt Pharmaceuticals, Medulary Thyroid Cancer Consortium (AstraZeneca Pharmaceuticals LP, Eli Lilly and Company, Novo Nordisk Inc, GlaxoSmithKline LLC), Merck Research Laboratories, Nektar Therapeutics Inc, NovoNordisk, Pacira Pharmaceuticals Inc, PTC Therapeutics Inc, Purdue Pharma LP, Sage Therapeutics, Sanofi US Services Inc, Shire Human Genetic Therapies Inc, and Transdermal Immediate Release Fentanyl REMS (BioDelivery Sciences International Inc, Insys Therapeutics Inc, Mylan Inc, Par Pharmaceutical Inc, Sentynl Therapeutics Inc, SpecGX LLC [a wholly owned subsidiary of Mallinckrodt Inc], Teva Pharmaceuticals USA Inc, West Therapeutic Development LLC). In addition, S. Hennessy leads the Center for Pharmacoepidemiology Research and Training, which has received support for pharmacoepidemiology training programs from Pfizer Inc. A. Zuppa has served on an advisory committee for Pfizer. All remaining authors have nothing to disclose.
Figures
Comment in
-
Renal Safety of Nonsteroidal Anti-Inflammatory Drugs and Opioids in Hospitalized Patients on Renin-Angiotensin System Inhibitors.Kidney360. 2020 Jul 20;1(7):586-587. doi: 10.34067/KID.0003682020. eCollection 2020 Jul 30. Kidney360. 2020. PMID: 35372946 Free PMC article. No abstract available.
References
-
- Wu CL, King AB, Geiger TM, Grant MC, Grocott MPW, Gupta R, Hah JM, Miller TE, Shaw AD, Gan TJ, Thacker JKM, Mythen MG, McEvoy MD; Fourth Perioperative Quality Initiative Workgroup : American society for enhanced recovery and perioperative quality initiative joint consensus statement on perioperative opioid minimization in opioid-naïve patients. Anesth Analg 129: 567–577, 2019 - PMC - PubMed
-
- Chou R, Gordon DB, de Leon-Casasola OA, Rosenberg JM, Bickler S, Brennan T, Carter T, Cassidy CL, Chittenden EH, Degenhardt E, Griffith S, Manworren R, McCarberg B, Montgomery R, Murphy J, Perkal MF, Suresh S, Sluka K, Strassels S, Thirlby R, Viscusi E, Walco GA, Warner L, Weisman SJ, Wu CL: Management of postoperative pain: A clinical practice guideline from the American pain society, the American society of regional anesthesia and pain medicine, and the American society of anesthesiologists’ committee on regional anesthesia, executive committee, and administrative council [published correction appears in J Pain 17: 508–510, 2016]. J Pain 17: 131–157, 2016 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
