

Insights into disparities observed with COVID-19
- PMID: 33164230
- PMCID: PMC9325576
- DOI: 10.1111/joim.13199
Insights into disparities observed with COVID-19
Abstract
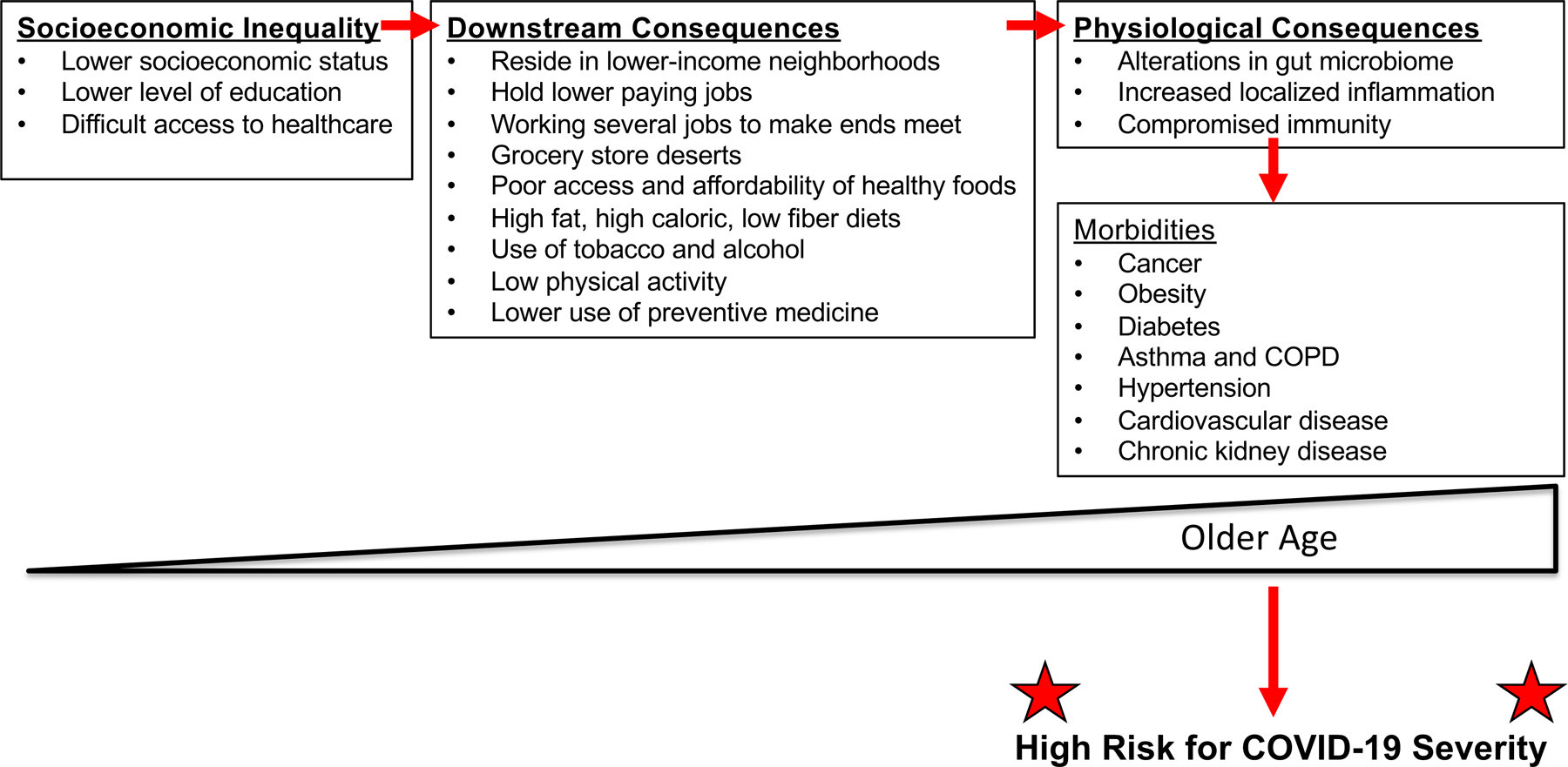
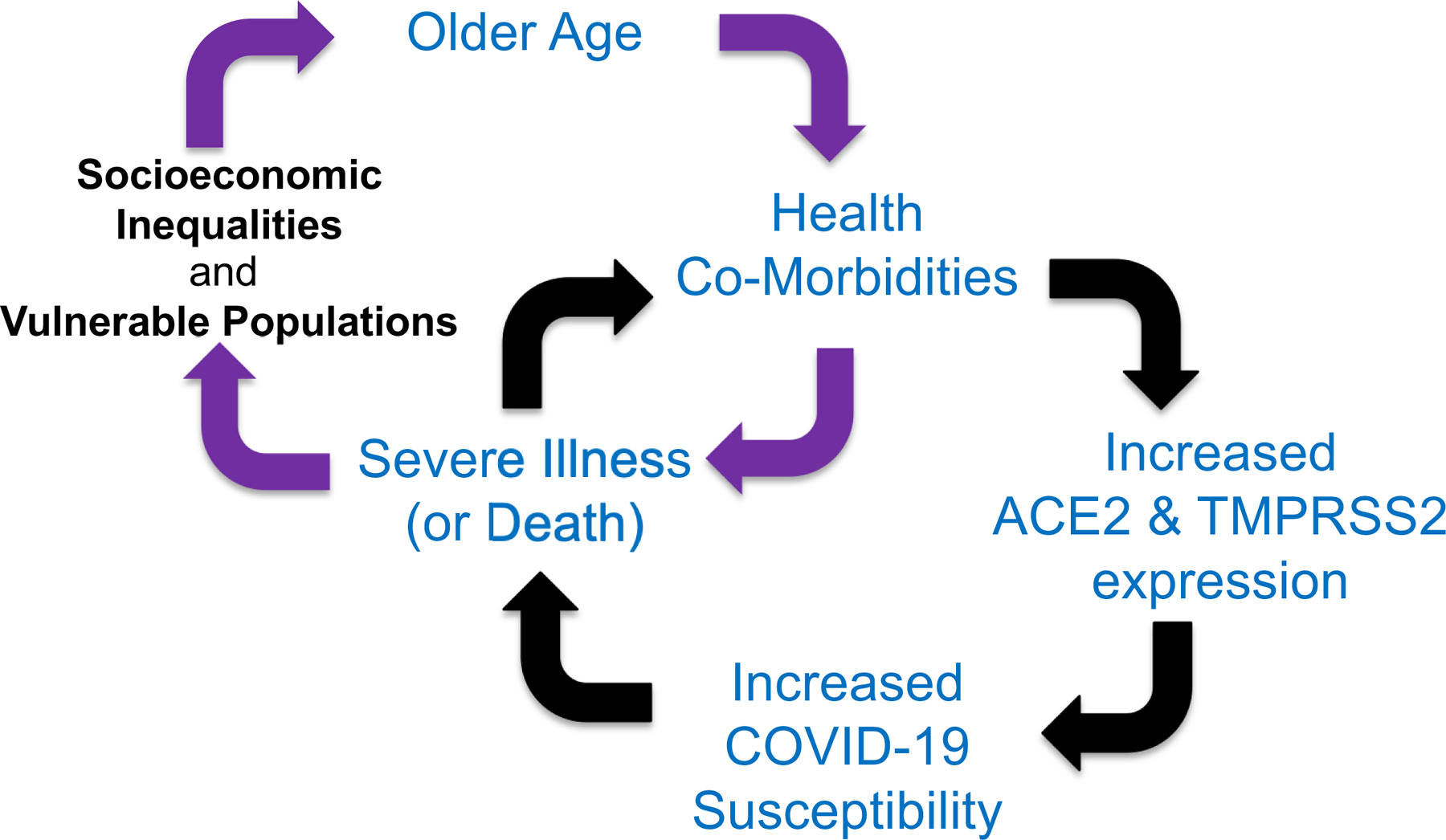
The onset of human disease by infection with SARS-CoV-2 causing COVID-19 has revealed risk factors for disease severity. There are four identified factors that put one at high risk for infection and/or mortality creating a disparity: age, co-morbidities, race/ethnicity and gender. Data indicate that the older a person is, and/or the presence of obesity and diabetes, cardiovascular disease and chronic kidney disease place one at higher risk for COVID-19. In the United States, specific race/ethnicities, particularly African Americans and Native Americans, are strong COVID-19 risk components. Male gender has also emerged as a severity risk factor. For age and racial/ethnicities, the accumulation of health co-morbidities is common precipitating mechanisms. In particular, underlying socio-economic structures in the United States likely drive development of co-morbidities, putting affected populations at higher risk for severe COVID-19. Sudden cardiac death triggered by a common sodium channel variant in African Americans with COVID-19 has not been evaluated as a cause for racial disparity. There is no evidence that racial/ethnic differences for COVID-19 are caused by ABO blood groups, use of angiotensin-converting enzyme (ACE) inhibitors or from amino acid substitutions in the SARS-CoV-2 spike protein. There is growing evidence that androgen-enabled expression of ACE2 receptors and the serine protease TMPRSS2, two permissive elements engaging the SARS-CoV-2 spike protein for infection, may contribute to severe COVID-19 in men. Overall, COVID-19 has generated disparities for who is infected and the severity of that infection. Understanding the mechanisms for the disparity will help nullify the differences in risk for COVID-19.
Keywords: ACE2; African American; COVID-19; Hispanic/Latinx; SARS-CoV-2; TMPRSS2; age; androgen; chronic kidney disease; co-morbidity; diabetes; disparity; ethnicity; hypertension; race.
© 2020 The Association for the Publication of the Journal of Internal Medicine.
Conflict of interest statement
Figures
References
-
- Matheson NJ, Lehner PJ. How does SARS-CoV-2 cause COVID-19? Science 2020;369:510–511. - PubMed
-
- Sungnak W, Huang N, Bécavin C, Berg M, Queen R, Litvinukova M, Talavera-López C, Maatz H, Reichart D, Sampaziotis F, Worlock KB, Yoshida M, Barnes JL; HCA Lung Biological Network. SARS-CoV-2 entry factors are highly expressed in nasal epithelial cells together with innate immune genes. Nat Med 2020;26:681–987. - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
