

Risk Factors for Delirium and Cognitive Decline Following Coronary Artery Bypass Grafting Surgery: A Systematic Review and Meta-Analysis
- PMID: 33164631
- PMCID: PMC7763731
- DOI: 10.1161/JAHA.120.017275
Risk Factors for Delirium and Cognitive Decline Following Coronary Artery Bypass Grafting Surgery: A Systematic Review and Meta-Analysis
Abstract
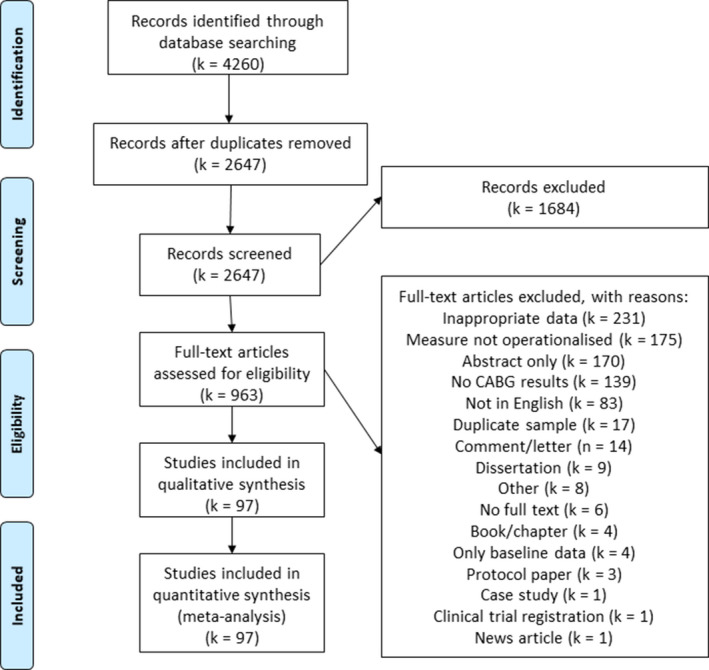
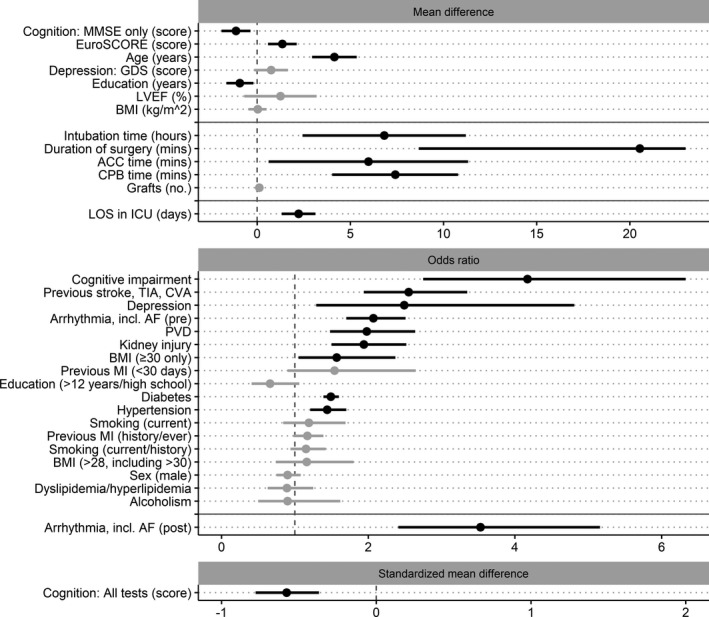
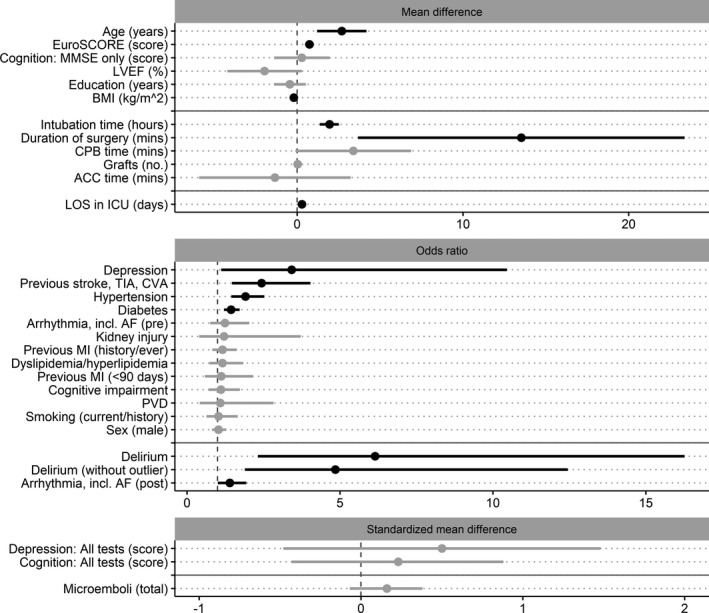
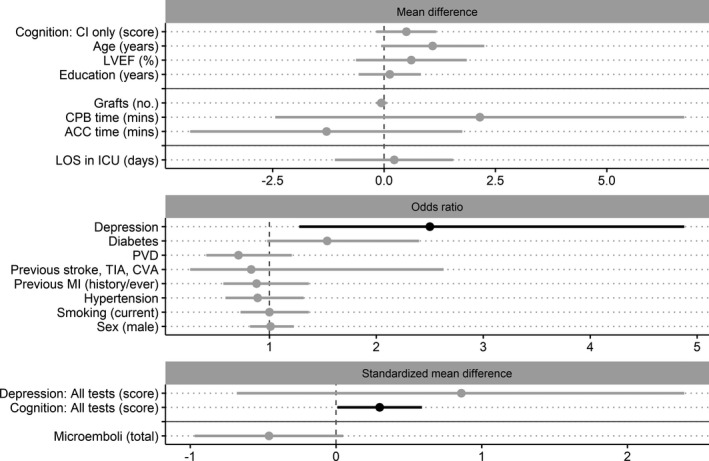
Background Coronary artery bypass grafting (CABG) is known to improve heart function and quality of life, while rates of surgery-related mortality are low. However, delirium and cognitive decline are common complications. We sought to identify preoperative, intraoperative, and postoperative risk or protective factors associated with delirium and cognitive decline (across time) in patients undergoing CABG. Methods and Results We conducted a systematic search of Medline, PsycINFO, EMBASE, and Cochrane (March 26, 2019) for peer-reviewed, English publications reporting post-CABG delirium or cognitive decline data, for at least one risk factor. Random-effects meta-analyses estimated pooled odds ratio for categorical data and mean difference or standardized mean difference for continuous data. Ninety-seven studies, comprising data from 60 479 patients who underwent CABG, were included. Moderate to large and statistically significant risk factors for delirium were as follows: (1) preoperative cognitive impairment, depression, stroke history, and higher European System for Cardiac Operative Risk Evaluation (EuroSCORE) score, (2) intraoperative increase in intubation time, and (3) postoperative presence of arrythmia and increased days in the intensive care unit; higher preoperative cognitive performance was protective for delirium. Moderate to large and statistically significant risk factors for acute cognitive decline were as follows: (1) preoperative depression and older age, (2) intraoperative increase in intubation time, and (3) postoperative presence of delirium and increased days in the intensive care unit. Presence of depression preoperatively was a moderate risk factor for midterm (1-6 months) post-CABG cognitive decline. Conclusions This meta-analysis identified several key risk factors for delirium and cognitive decline following CABG, most of which are nonmodifiable. Future research should target preoperative risk factors, such as depression or cognitive impairment, which are potentially modifiable. Registration URL: https://www.crd.york.ac.uk/prospero/; Unique identifier: CRD42020149276.
Keywords: cognitive decline; coronary artery bypass grafting; delirium; meta‐analysis.
Conflict of interest statement
None.
Figures
References
-
- Head S, Milojevic M, Taggart D, Puskas J. Current practice of state‐of-the‐art surgical coronary revascularization. Circulation. 2017;136:1331–1345. - PubMed
-
- Newman M, Kirchner J, Phillips‐Bute B, Gaver V, Grocott H, Jones R, Mark D, Reves J, Blumenthal J. Longitudinal assessment of neurocognitive function after coronary‐artery bypass surgery. N Engl J Med. 2001;344:395–402. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
