

Improved chemosensitivity following mucolytic therapy in patient-derived models of mucinous appendix cancer
- PMID: 33164812
- PMCID: PMC7867596
- DOI: 10.1016/j.trsl.2020.10.005
Improved chemosensitivity following mucolytic therapy in patient-derived models of mucinous appendix cancer
Abstract
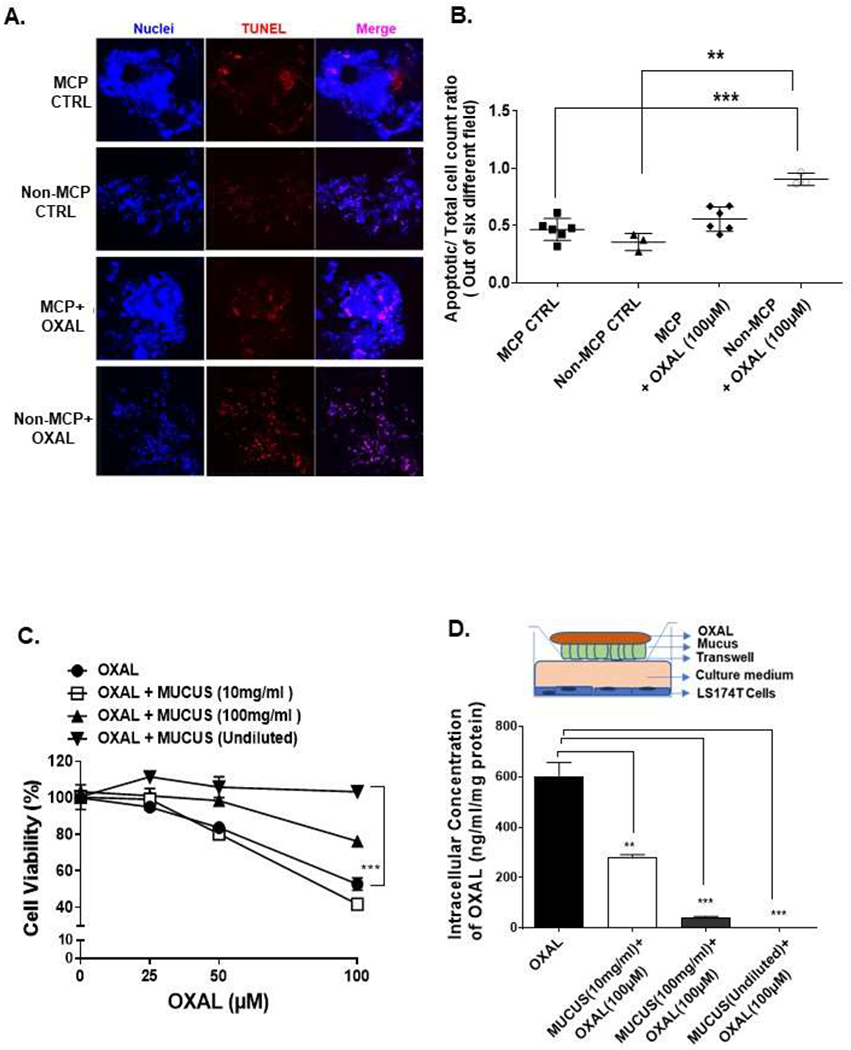
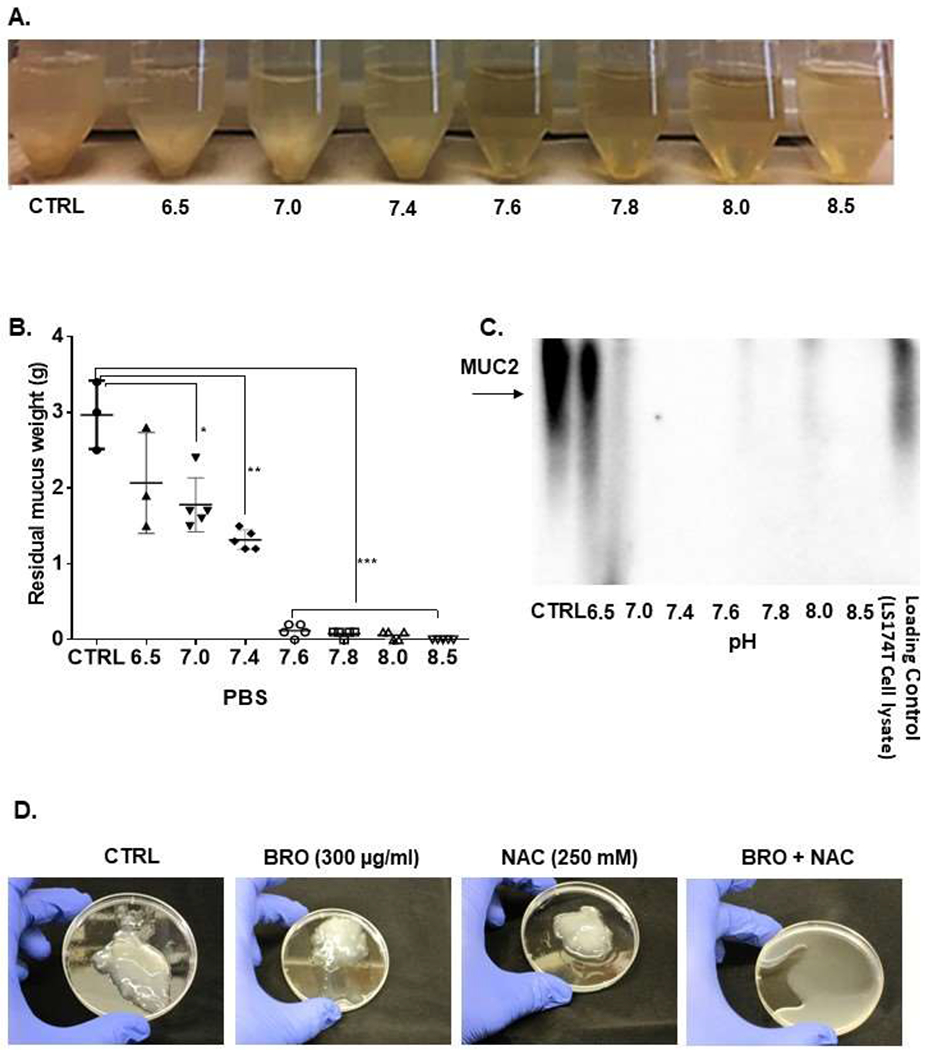
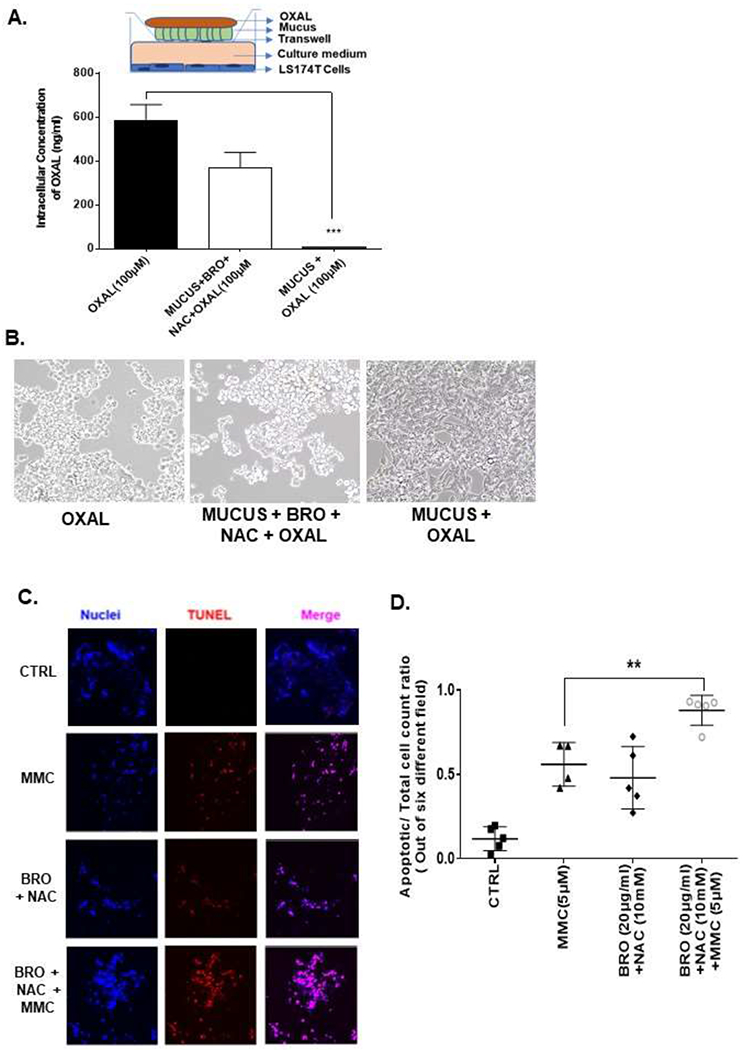
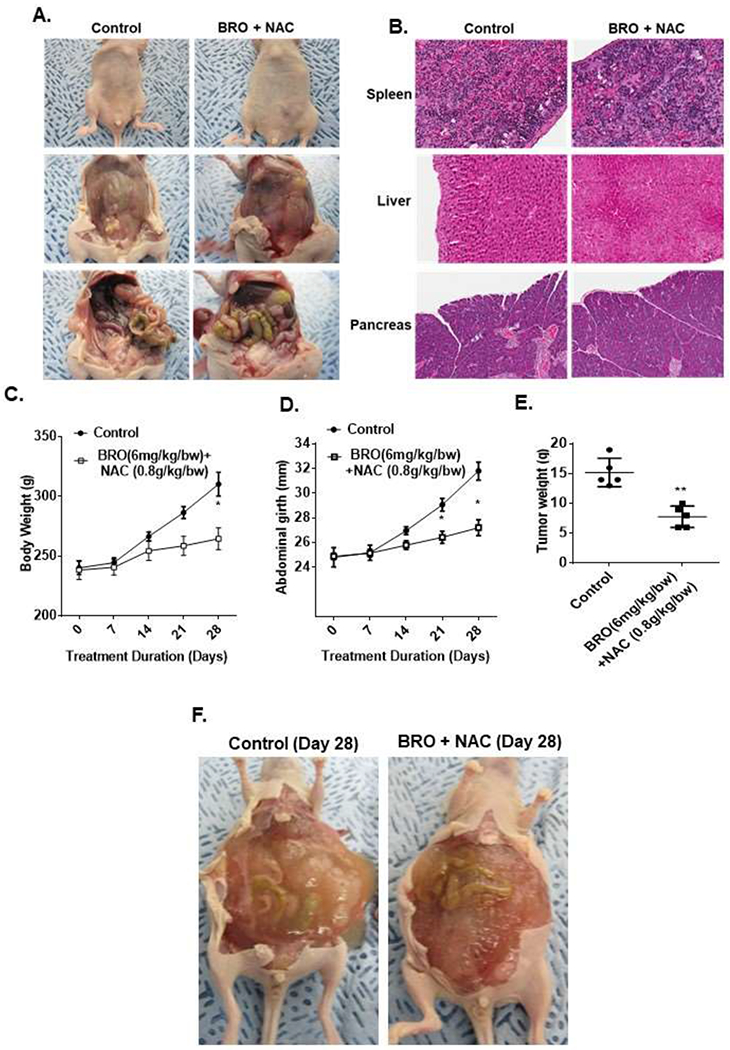
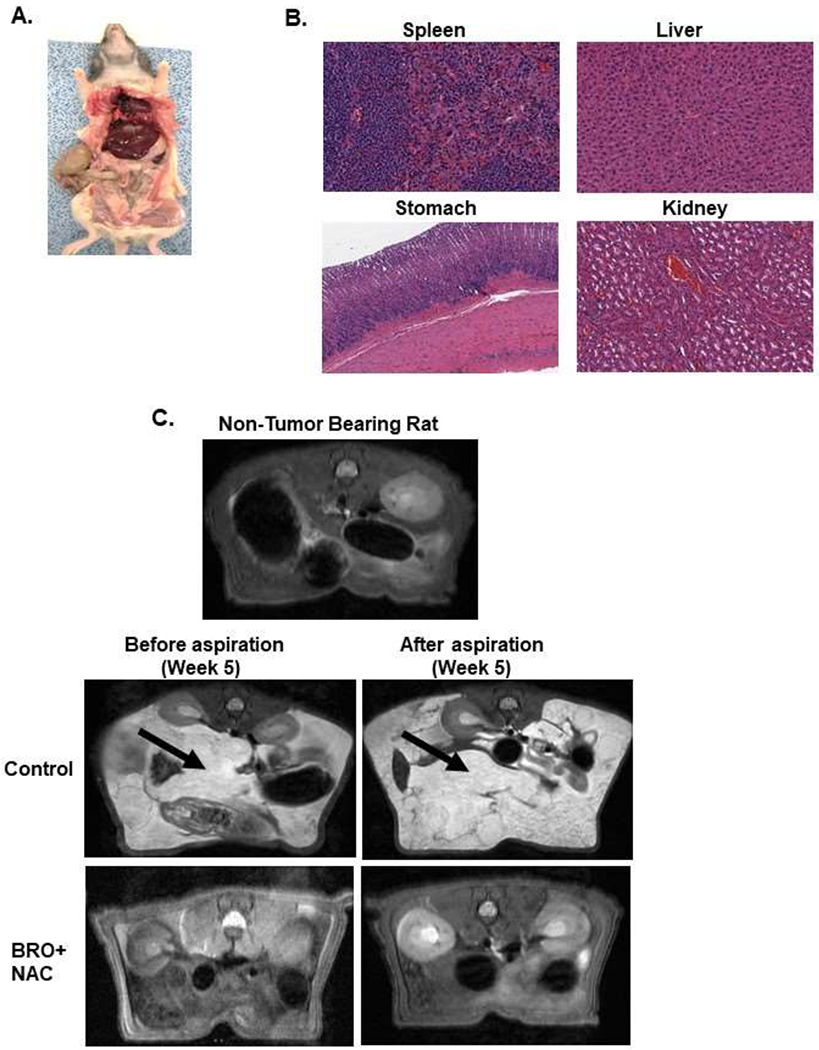
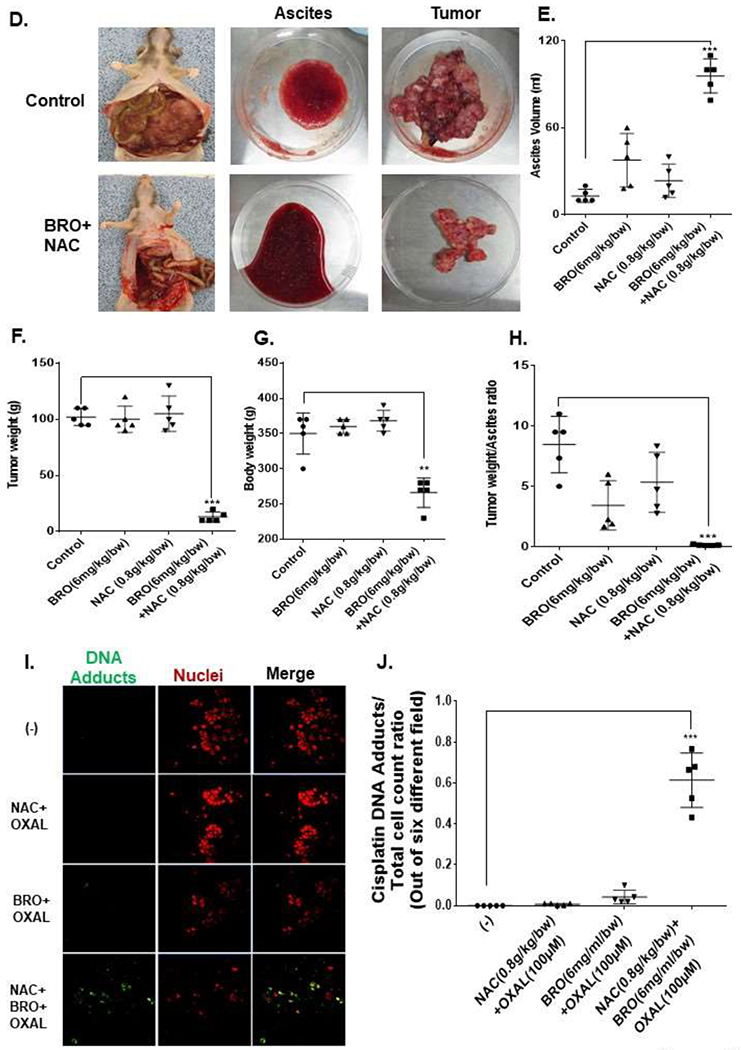
Abundant intraperitoneal (IP) accumulation of extracellular mucus in patients with appendiceal mucinous carcinoma peritonei (MCP) causes compressive organ dysfunction and prevents delivery of chemotherapeutic drugs to cancer cells. We hypothesized that reducing extracellular mucus would decrease tumor-related symptoms and improve chemotherapeutic effect in patient-derived models of MCP. Mucolysis was achieved using a combination of bromelain (BRO) and N-acetylcysteine (NAC). Ex vivo experiments of mucolysis and chemotherapeutic drug delivery/effect were conducted with MCP and non-MCP tissue explants. In vivo experiments were performed in mouse and rat patient-derived xenograft (PDX) models of early and late (advanced) MCP. MCP tumor explants were less chemosensitive than non-MCP explants. Chronic IP administration of BRO + NAC in a mouse PDX model of early MCP and a rat PDX model of late (advanced) MCP converted solid mucinous tumors into mucinous ascites (mucolysis) that could be drained via a percutaneous catheter (rat model only), significantly reduced solid mucinous tumor growth and improved the efficacy of chemotherapeutic drugs. Combination of BRO + NAC efficiently lyses extracellular mucus in clinically relevant models of MCP. Conversion of solid mucinous tumors into mucinous ascites decreases tumor bulk and allows for minimally invasive drainage of liquified tumors. Lysis of extracellular mucus removes the protective mucinous coating surrounding cancer cells and improves chemotherapeutic drug delivery/efficacy in cancer cells. Our data provide a preclinical rationale for the clinical evaluation of BRO + NAC as a therapeutic strategy for MCP.
Copyright © 2020 Elsevier Inc. All rights reserved.
Conflict of interest statement
Conflict of Interest: All authors have read the journals policy on disclosure of potential conflicts, and have no competing interests to declare. All authors have read the journal’s authorship agreement, and approved the final version of the manuscript.
Figures
References
-
- Hugen N, Brown G, Glynne-Jones R, de Wilt JH, Nagtegaal ID. Advances in the care of patients with mucinous colorectal cancer. Nat Rev Clin Oncol. 2016;13(6):361–9. - PubMed
-
- O’Connell JT, Hacker CM, Barsky SH. MUC2 is a molecular marker for pseudomyxoma peritonei. Mod Pathol. 2002;15(9):958–72. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
