

Artificial Intelligence-Powered Smartphone App to Facilitate Medication Adherence: Protocol for a Human Factors Design Study
- PMID: 33164898
- PMCID: PMC7683257
- DOI: 10.2196/21659
Artificial Intelligence-Powered Smartphone App to Facilitate Medication Adherence: Protocol for a Human Factors Design Study
Abstract
Background: Medication Guides consisting of crucial interactions and side effects are extensive and complex. Due to the exhaustive information, patients do not retain the necessary medication information, which can result in hospitalizations and medication nonadherence. A gap exists in understanding patients' cognition of managing complex medication information. However, advancements in technology and artificial intelligence (AI) allow us to understand patient cognitive processes to design an app to better provide important medication information to patients.
Objective: Our objective is to improve the design of an innovative AI- and human factor-based interface that supports patients' medication information comprehension that could potentially improve medication adherence.
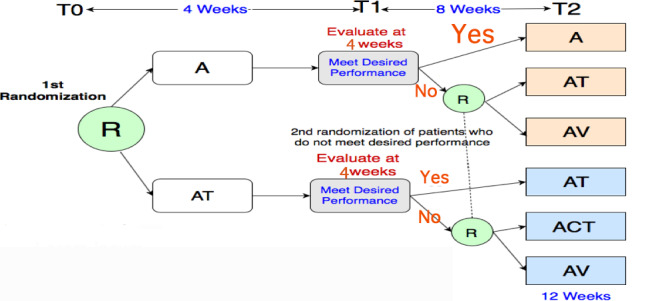
Methods: This study has three aims. Aim 1 has three phases: (1) an observational study to understand patient perception of fear and biases regarding medication information, (2) an eye-tracking study to understand the attention locus for medication information, and (3) a psychological refractory period (PRP) paradigm study to understand functionalities. Observational data will be collected, such as audio and video recordings, gaze mapping, and time from PRP. A total of 50 patients, aged 18-65 years, who started at least one new medication, for which we developed visualization information, and who have a cognitive status of 34 during cognitive screening using the TICS-M test and health literacy level will be included in this aim of the study. In Aim 2, we will iteratively design and evaluate an AI-powered medication information visualization interface as a smartphone app with the knowledge gained from each component of Aim 1. The interface will be assessed through two usability surveys. A total of 300 patients, aged 18-65 years, with diabetes, cardiovascular diseases, or mental health disorders, will be recruited for the surveys. Data from the surveys will be analyzed through exploratory factor analysis. In Aim 3, in order to test the prototype, there will be a two-arm study design. This aim will include 900 patients, aged 18-65 years, with internet access, without any cognitive impairment, and with at least two medications. Patients will be sequentially randomized. Three surveys will be used to assess the primary outcome of medication information comprehension and the secondary outcome of medication adherence at 12 weeks.
Results: Preliminary data collection will be conducted in 2021, and results are expected to be published in 2022.
Conclusions: This study will lead the future of AI-based, innovative, digital interface design and aid in improving medication comprehension, which may improve medication adherence. The results from this study will also open up future research opportunities in understanding how patients manage complex medication information and will inform the format and design for innovative, AI-powered digital interfaces for Medication Guides.
International registered report identifier (irrid): PRR1-10.2196/21659.
Keywords: artificial intelligence; complex medication information; machine learning; medication adherence; mobile phone; patient cognition; smartphone app.
©Don Roosan, Jay Chok, Mazharul Karim, Anandi V Law, Andrius Baskys, Angela Hwang, Moom R Roosan. Originally published in JMIR Research Protocols (http://www.researchprotocols.org), 09.11.2020.
Conflict of interest statement
Conflicts of Interest: None declared.
Figures
References
-
- Cunningham MR. Revolutionizing the patient package insert with infographics. BU Well. 2016 May 13;1:5–6.
-
- Wolf MS, King J, Wilson EAH, Curtis LM, Bailey SC, Duhig J, Russell A, Bergeron A, Daly A, Parker RM, Davis TC, Shrank WH, Lambert B. Usability of FDA-approved Medication Guides. J Gen Intern Med. 2012 Dec;27(12):1714–1720. doi: 10.1007/s11606-012-2068-7. http://europepmc.org/abstract/MED/22566170 - DOI - PMC - PubMed
-
- Hoy MG, Levenshus AB. A mixed-methods approach to assessing actual risk readership on branded drug websites. J Risk Res. 2016 Aug 27;21(5):521–538. doi: 10.1080/13669877.2016.1223160. - DOI
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
