

Perioperative Blood Transfusions Are Associated with a Higher Incidence of Thromboembolic Events After TKA: An Analysis of 333,463 TKAs
- PMID: 33165044
- PMCID: PMC7899570
- DOI: 10.1097/CORR.0000000000001513
Perioperative Blood Transfusions Are Associated with a Higher Incidence of Thromboembolic Events After TKA: An Analysis of 333,463 TKAs
Abstract
Background: Given the morbidity, mortality, and financial burden associated with venous thromboembolism (VTE) after TKA, orthopaedic providers continually seek to identify risk factors associated with this devastating complication. The association between perioperative transfusion status and VTE risk has not been thoroughly explored, with previous studies evaluating this relationship being limited in both generalizability and power.
Questions/purposes: Therefore, we sought to determine whether perioperative transfusions were associated with an increased risk of (1) pulmonary embolism (PE) or (2) deep vein thrombosis (DVT) after primary TKA in a large, multi-institutional sample.
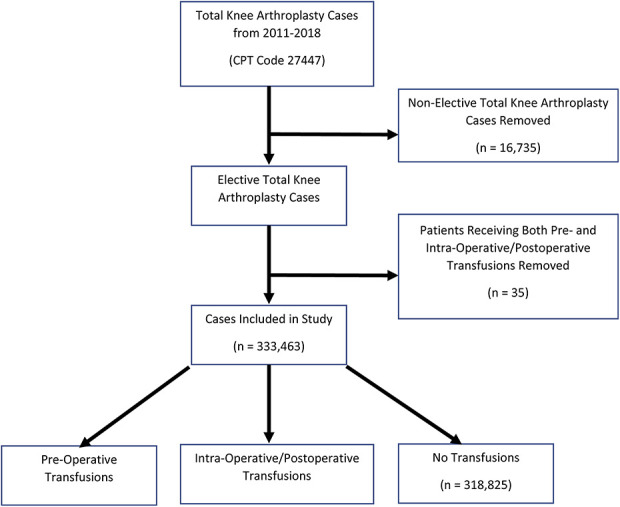
Methods: The American College of Surgeons National Surgical Quality Improvement Program (ACS NSQIP) database was implemented for our analysis. The definitions of complications, such as DVT and PE, and risk adjustment validation is monitored by the central ACS NSQIP office to ensure participating hospitals are adhering to the same guidelines to log patients. Additionally, both preoperative and intraoperative/72 hour postoperative transfusion status is included for all patients. Therefore, ACS NSQIP was determined to be the most appropriate database for our analysis. All patients who underwent primary TKA between 2011 and 2018 were identified using Current Procedural Terminology code 27447. Primary TKAs designated as "non-elective" were excluded, thereby providing a cohort composed solely of patients undergoing unilateral primary elective TKA for further analysis. The final analysis included 333,463 patients undergoing TKA (mean age 67 ± 9 years, 62% female). Preoperative transfusions were received by < 0.01% (48 of 333,463) of the patients, while 4% (14,590 of 333,463) received a transfusion within the interim between the start of surgery up to 72 hours postoperatively. All missing values were imputed through multiple imputation by chained equation to avoid variable availability-based selection and the subsequent listwise deletion-associated bias in the estimate of parameters. A multivariable logistic regression analysis was conducted using variables identified in a univariate model to calculate adjusted odds ratios and 95% confidence intervals for risk factors associated with symptomatic DVT and/or PE. For variables that maintained significance in the multivariable model, an additional model without confounders was used to generate fully adjusted ORs and 95% CIs. A propensity score matched comparison between recipients versus nonrecipients (1:1) of transfusion (preoperative and intraoperative/72 hours postoperative) was then conducted to evaluate the independent association between DVT/PE development and patients' transfusion status. Significance was determined at a p value < 0.05.
Results: Adjusted multivariable regression analysis accounting for patient age, sex, race, BMI, American Society of Anesthesiologists (ASA) class and baseline comorbidities demonstrated the absence of an association between preoperative (OR 1.75 [95% CI 0.24 to 12.7]; p = 0.58) or intraoperative/72 hours postoperative (OR 1.12 [95% CI 0.93 to 1.35]; p = 0.23) transfusions and higher odds of developing PE. Similar findings were demonstrated after propensity score matching. Although multivariable regression demonstrated the absence of an association between preoperative transfusion and the odds of developing DVT within the 30-day postoperative period (OR 1.85 [95% CI 0.43 to 8.05]; p = 0.41), intraoperative/postoperative transfusion was associated with higher odds of DVT development (OR 3.68 [95% CI 1.14 to 1.53]; p < 0.001) relative to transfusion naïve patients. However, this significance was lost after propensity score matching.
Conclusion: After controlling for various potential confounding variables such as ASA Class, age, anesthesia type, and BMI, the receipt of an intra- or postoperative transfusion was found to be associated with an increased risk of DVT. Our findings should encourage orthopaedic providers to strictly adhere to blood management protocols, further tighten transfusion eligibility, and adjust surgical approach and implant type to reduce the incidence of transfusion among patients with other DVT risk factors. Additionally, our findings should encourage a multidisciplinary approach to VTE prophylaxis and prevention, as well as to blood transfusion guideline adherence, among all providers of the care team.
Level of evidence: Level III, therapeutic study.
Copyright © 2020 by the Association of Bone and Joint Surgeons.
Conflict of interest statement
Each remaining author certifies that neither he, nor any member of immediate family, has funding or commercial associations (consultancies, stock ownership, equity interest, patent/licensing arrangements, etc.) that might pose a conflict of interest in connection with the submitted article. All ICMJE Conflict of Interest Forms for authors and Clinical Orthopaedics and Related Research® editors and board members are on file with the publication and can be viewed on request.
Figures
References
-
- Anderson DR, Dunbar M, Murnaghan J, Kahn SR, Gross P, Forsythe M, Pelet S, Fisher W, Belzile E, Dolan S, Crowther M, Bohm E, MacDonald SJ, Gofton W, Kim P, Zukor D, Pleasance S, Andreou P, Doucette S, Theriault C, Abianui A, Carrier M, Kovacs MJ, Rodger MA, Coyle D, Wells PS, Vendittoli P-A. Aspirin or rivaroxaban for VTE prophylaxis after hip or knee arthroplasty. N Engl J Med. 2018;378:699–707. - PubMed
-
- Bateman DK, Dow RW, Brzezinski A, Bar-Eli HY, Kayiaros ST. Correlation of the Caprini score and venous thromboembolism incidence following primary total joint arthroplasty—Results of a single-institution protocol. J Arthroplasty. 2017;32:3735–3741. - PubMed
-
- Bielby L, Moss R, Mo A, McQuilten Z, Wood E. The role of the transfusion practitioner in the management of anaemia. ISBT Sci Ser. 2020;15:82–90.
-
- Bjørnarå BT, Gudmundsen TE, Dahl OE. Frequency and timing of clinical venous thromboembolism after major joint surgery. J Bone Joint Surg Br. 2006;88:386–391. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
