

What Are the Frequency, Related Mortality, and Factors Associated with Bone Cement Implantation Syndrome in Arthroplasty Surgery?
- PMID: 33165048
- PMCID: PMC8083844
- DOI: 10.1097/CORR.0000000000001541
What Are the Frequency, Related Mortality, and Factors Associated with Bone Cement Implantation Syndrome in Arthroplasty Surgery?
Abstract
Background: Bone cement implantation syndrome (BCIS) is characterized by hypoxia, hypotension, and the loss of consciousness during cemented arthroplasty; it may result in death. Its incidence has only been explored for hemiarthroplasty and THA after fracture or cancer. To our knowledge, there are no studies that comprehensively explore and compare the incidence of BCIS in other arthroplasty procedures.
Questions/purposes: (1) To report the incidence of BCIS in TKA, unicondylar knee arthroplasty, hip hemiarthroplasty, THA, shoulder arthroplasty, TKA, and revision THA and TKA; (2) to determine whether severe BCIS is associated with an increased risk of death within 30 days of surgery; and (3) to identify factors associated with the development of severe BCIS.
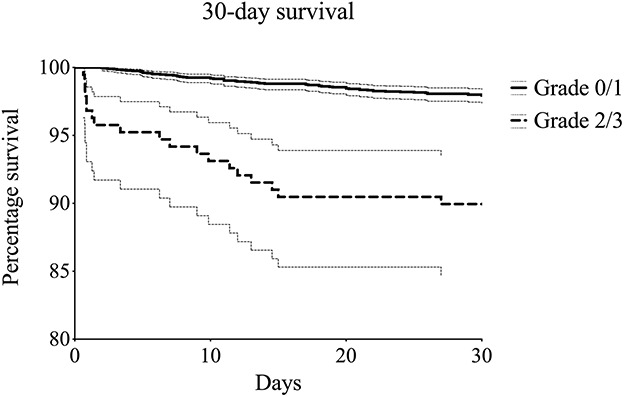
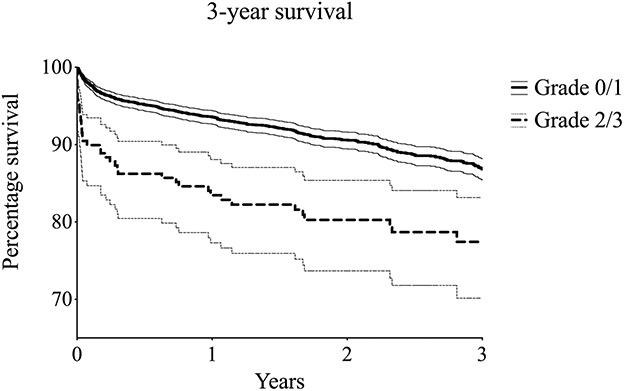
Methods: All patients undergoing cemented arthroplasty for any reason (TKA [11% cemented, 766 of 7293], unicondylar knee arthroplasty [100% cemented, 562 procedures], hip hemiarthroplasty for femur fractures [100% cemented, 969 procedures], THA [8% cemented, 683 of 8447], shoulder arthroplasty [84% cemented, 185 of 219], and revision arthroplasty of the hip and knee [36% cemented, 240 of 660]) between January 2008 and August 2019 were considered for inclusion in the current retrospective observational study. Fixation choice was dependent on surgeon preference (THA and TKA), prosthesis design (shoulder arthroplasty), or bone quality (revision arthroplasty). The following procedures were excluded because of insufficient data: < 1% (1 of 766) of TKAs, 1% (4 of 562) of unicondylar knee arthroplasties, 6% (54 of 969) of hip hemiarthroplasties, 1% (6 of 683) of THAs, 6% (12 of 185) of shoulder arthroplasties, and 14% (34 of 240) of revision procedures. This resulted in a final inclusion of 3294 procedures (765 TKAs [23%], 558 unicondylar knee arthroplasties [17%], 915 hip hemiarthroplasties [28%], 677 THA [21%], 173 shoulder arthroplasties [5%], and 206 revision arthroplasties [6%]), of which 28% (930 of 3294) had an emergent indication for surgery. Of the patients, 68% (2240 of 3294) were females, with a mean age of 75 ± 11 years. All anesthetic records were extracted from our hospital's database, and the severity of BCIS was retrospectively scored (Grade 0 [no BCIS], Grade 1 [O2% < 94% or fall in systolic blood pressure of 20% to 40%], Grade 2 [O2% < 88% or fall in systolic blood pressure of > 40%], and Grade 3 [cardiovascular collapse requiring CPR]). Procedures were dichotomized into no or moderate BCIS (Grades 0 and 1) and severe BCIS (Grades 2 and 3). The adjusted 30-day mortality of patients with severe BCIS was assessed with a multivariate Cox regression analysis. A multivariate logistic regression analysis was performed to identify factors associated with the development of severe BCIS.
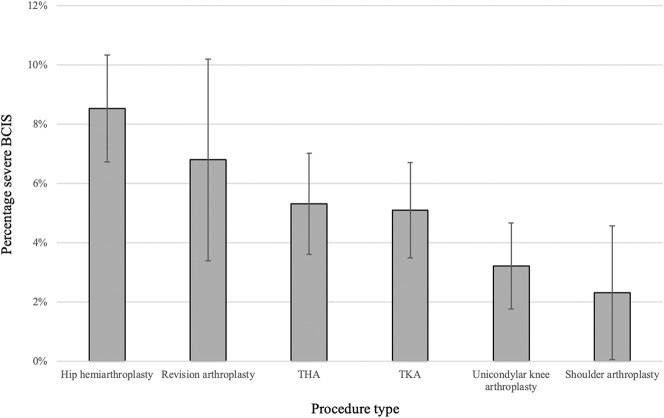
Results: BCIS occurred in 26% (845 of 3294) of arthoplasty procedures. The incidence was 31% (282 of 915) in hip hemiarthroplasty, 28% (210 of 765) in TKA, 24% (165 of 677) in THA, 23% (47 of 206) in revision arthroplasty, 20% (113 of 558) in unicondylar knee arthroplasty, and 16% (28 of 173) in shoulder arthroplasty. Patients with severe BCIS were more likely (hazard ratio 3.46 [95% confidence interval 2.07 to 5.77]; p < 0.001) to die within 30 days of the index procedure than were patients with less severe or no BCIS. Factors independently associated with the development of severe BCIS were age older than 75 years (odds ratio 1.57 [95% CI 1.09 to 2.27]; p = 0.02), American Society of Anesthesiologists Class III or IV (OR 1.58 [95% CI 1.09 to 2.30]; p = 0.02), and renal impairment (OR 3.32 [95% CI 1.45 to 7.46]; p = 0.004).
Conclusion: BCIS is common during cemented arthroplasty; severe BCIS is uncommon, but it is associated with an increased risk of death within 30 days of surgery. Medically complex patients undergoing hip hemiarthroplasty may be at particular risk. Patients at high risk for severe BCIS (renal impairment, ASA III/IV, and age older than 75 years) should be identified and preventive measures such as medullary lavage before cementation, femoral venting, and avoidance of excessive pressurization of implants should be taken to reduce the likelihood and consequences of BCIS. Because of the increased risk of periprosthetic fractures in uncemented hip stems, factors associated with the development of BCIS should be weighed against the risk factors for sustaining periprosthetic fractures (poor bone quality, female sex) to balance the risks of fixation method against those of BCIS for each patient.
Level of evidence: Level III, therapeutic study.
Copyright © 2020 by the Association of Bone and Joint Surgeons.
Conflict of interest statement
Each author certifies that he nor she, nor any member of his or her immediate family, has funding or commercial associations (consultancies, stock ownership, equity interest, patent/licensing arrangements, etc.) that might pose a conflict of interest in connection with the submitted article. All ICMJE Conflict of Interest Forms for authors and Clinical Orthopaedics and Related Research® editors and board members are on file with the publication and can be viewed on request.
Figures
Comment in
-
CORR Insights®: What Are the Frequency, Related Mortality, and Factors Associated with Bone Cement Implantation Syndrome in Arthroplasty Surgery?Clin Orthop Relat Res. 2021 Apr 1;479(4):764-766. doi: 10.1097/CORR.0000000000001658. Clin Orthop Relat Res. 2021. PMID: 33570859 Free PMC article. No abstract available.
References
-
- Bengtson A, Larsson M, Gammer W, Heideman M. Anaphylatoxin release in association with methylmethacrylate fixation of hip prostheses. J Bone Joint Surg Am. 1987;69:46-49. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
