

Cannula With Long and Narrow Tubing vs Short Binasal Prongs for Noninvasive Ventilation in Preterm Infants: Noninferiority Randomized Clinical Trial
- PMID: 33165539
- PMCID: PMC7653541
- DOI: 10.1001/jamapediatrics.2020.3579
Cannula With Long and Narrow Tubing vs Short Binasal Prongs for Noninvasive Ventilation in Preterm Infants: Noninferiority Randomized Clinical Trial
Abstract
Importance: Use of cannulas with long and narrow tubing (CLNT) has gained increasing popularity for applying noninvasive respiratory support for newborn infants thanks to ease of use, perceived patient comfort, and reduced nasal trauma. However, there is concern that this interface delivers reduced and suboptimal support.
Objective: To determine whether CLNT is noninferior to short binasal prongs and masks (SPM) when providing nasal intermittent positive pressure ventilation (NIPPV) in preterm infants.
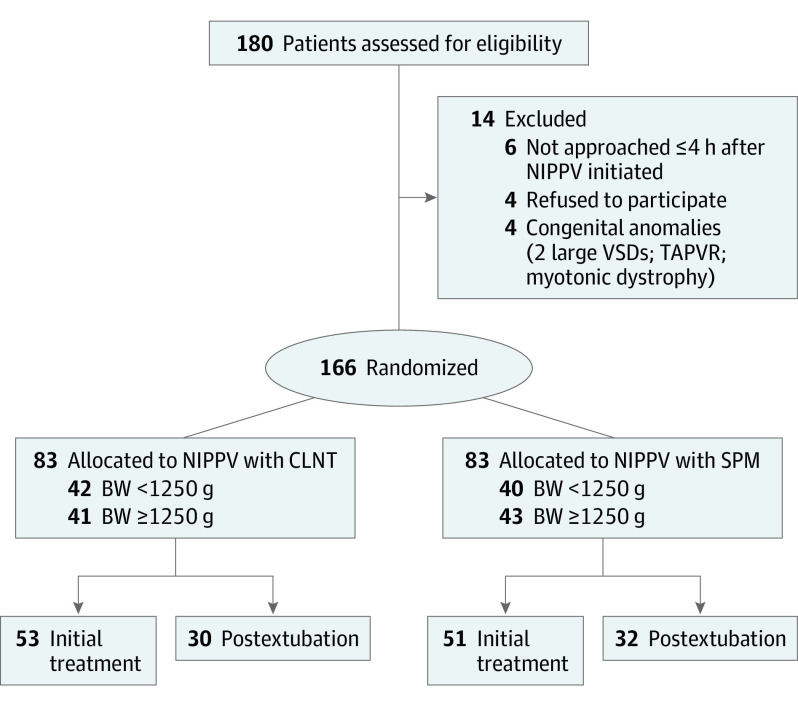
Design, setting, and participants: This randomized controlled, unblinded, prospective noninferiority trial was conducted between December 2017 and December 2019 at 2 tertiary neonatal intensive care units. Preterm infants born between 24 weeks' and 33 weeks and 6 days' gestation were eligible if presented with respiratory distress syndrome with the need for noninvasive ventilatory support either as initial treatment after birth or after first extubation. Analysis was performed by intention to treat.
Interventions: Randomization to NIPPV with either CLNT or SPM interface.
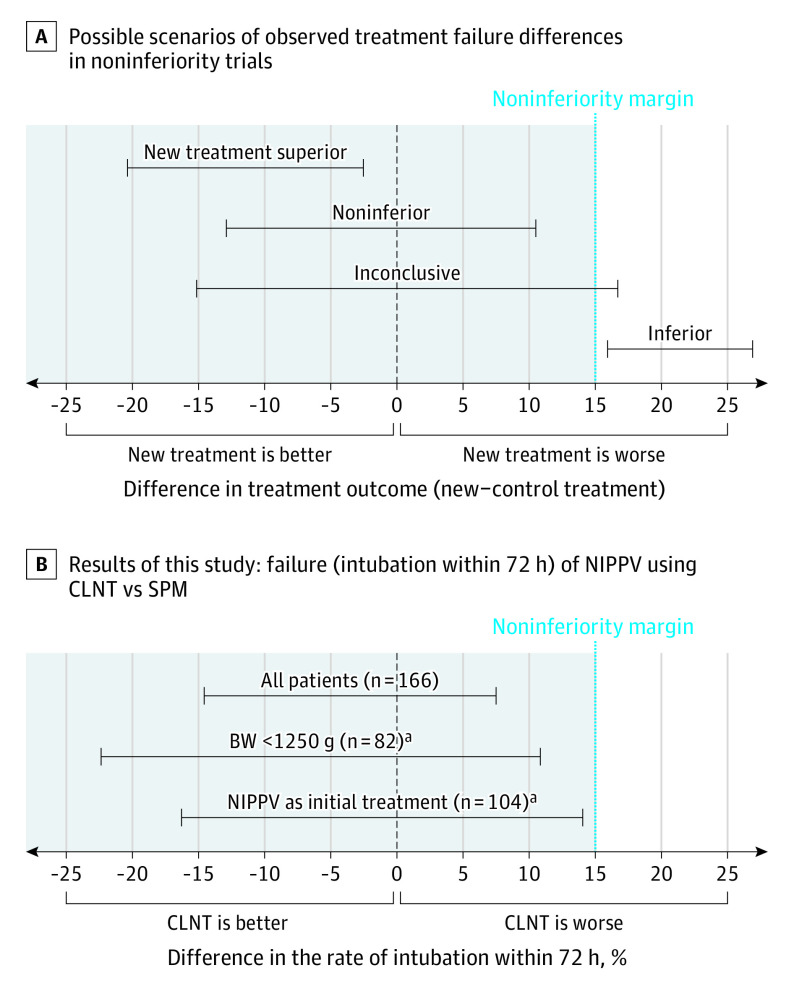
Main outcomes and measures: The primary outcome was the need for intubation within 72 hours after NIPPV treatment began. Noninferiority margin was defined as 15% or less absolute difference.
Results: Overall, 166 infants were included in this analysis, and infant characteristics and clinical condition (including fraction of inspired oxygen, Pco2, and pH level) were comparable at recruitment in the CLNT group (n = 83) and SPM group (n = 83). The mean (SD) gestational age was 29.3 (2.2) weeks vs 29.2 (2.5) weeks, and the mean (SD) birth weight was 1237 (414) g vs 1254 (448) g in the CLNT and SPM groups, respectively. Intubation within 72 hours occurred in 12 of 83 infants (14%) in the CLNT group and in 15 of 83 infants (18%) in the SPM group (risk difference, -3.6%; 95% CI, -14.8 to 7.6 [within the noninferiority margin], χ2 P = .53). Moderate to severe nasal trauma was significantly less common in the CLNT group compared with the SPM group (4 [5%] vs 14 [17%]; P = .01). There were no differences in other adverse events or in the course during hospitalization.
Conclusions and relevance: In this study, CLNT was noninferior to SPM in providing NIPPV for preterm infants, while causing significantly less nasal trauma.
Trial registration: ClinicalTrials.gov Identifier: NCT03081611.
Conflict of interest statement
Figures
References
-
- LeVan JM, Brion LP, Wrage LA, et al. ; Eunice Kennedy Shriver NICHD Neonatal Research Network . Change in practice after the surfactant, positive pressure and oxygenation randomised trial. Arch Dis Child Fetal Neonatal Ed. 2014;99(5):F386-F390. doi: 10.1136/archdischild-2014-306057 - DOI - PMC - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
