

Mortality risk assessment in Spain and Italy, insights of the HOPE COVID-19 registry
- PMID: 33165755
- PMCID: PMC7649104
- DOI: 10.1007/s11739-020-02543-5
Mortality risk assessment in Spain and Italy, insights of the HOPE COVID-19 registry
Abstract
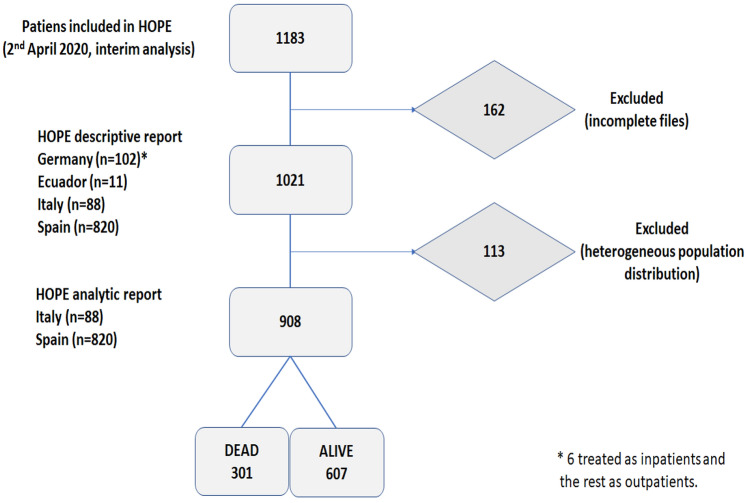
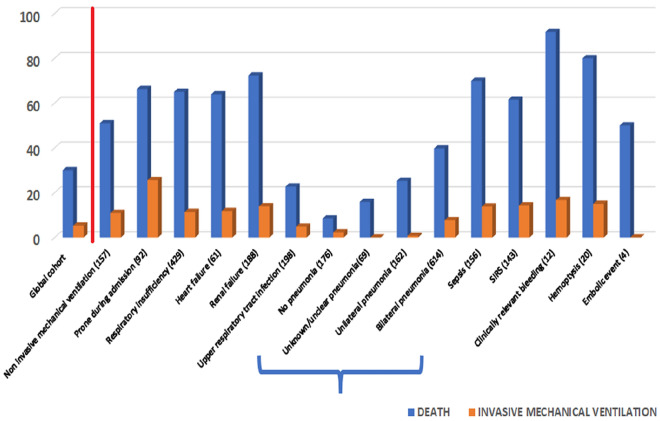
Recently the coronavirus disease (COVID-19) outbreak has been declared a pandemic. Despite its aggressive extension and significant morbidity and mortality, risk factors are poorly characterized outside China. We designed a registry, HOPE COVID-19 (NCT04334291), assessing data of 1021 patients discharged (dead or alive) after COVID-19, from 23 hospitals in 4 countries, between 8 February and 1 April. The primary end-point was all-cause mortality aiming to produce a mortality risk score calculator. The median age was 68 years (IQR 52-79), and 59.5% were male. Most frequent comorbidities were hypertension (46.8%) and dyslipidemia (35.8%). A relevant heart or lung disease were depicted in 20%. And renal, neurological, or oncological disease, respectively, were detected in nearly 10%. Most common symptoms were fever, cough, and dyspnea at admission. 311 patients died and 710 were discharged alive. In the death-multivariate analysis, raised as most relevant: age, hypertension, obesity, renal insufficiency, any immunosuppressive disease, 02 saturation < 92% and an elevated C reactive protein (AUC = 0.87; Hosmer-Lemeshow test, p > 0.999; bootstrap-optimist: 0.0018). We provide a simple clinical score to estimate probability of death, dividing patients in four grades (I-IV) of increasing probability. Hydroxychloroquine (79.2%) and antivirals (67.6%) were the specific drugs most commonly used. After a propensity score adjustment, the results suggested a slight improvement in mortality rates (adjusted-ORhydroxychloroquine 0.88; 95% CI 0.81-0.91, p = 0.005; adjusted-ORantiviral 0.94; 95% CI 0.87-1.01; p = 0.115). COVID-19 produces important mortality, mostly in patients with comorbidities with respiratory symptoms. Hydroxychloroquine could be associated with survival benefit, but this data need to be confirmed with further trials. Trial Registration: NCT04334291/EUPAS34399.
Keywords: COVID-19; Mortality; Prognosis; Registry; Score.
Conflict of interest statement
The author(s) declare that they have no conflict of interest.
Figures
References
-
- WHO. WHO statement regarding cluster of pneumonia cases in Wuhan, China. https://www.who.int/china/news/detail/09-01-2020-who-statement-regarding.... Accessed 27 Apr 2020
-
- WHO. https://www.euro.who.int/en/health-topics/health-emergencies/coronavirus.... Accessed 27 Apr 2020
-
- WHO. https://www.who.int/emergencies/diseases/novel-coronavirus-2019. Accesed 27 Apr 2020
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
