

Alkali supplementation as a therapeutic in chronic kidney disease: what mediates protection?
- PMID: 33166183
- PMCID: PMC7792697
- DOI: 10.1152/ajprenal.00343.2020
Alkali supplementation as a therapeutic in chronic kidney disease: what mediates protection?
Abstract
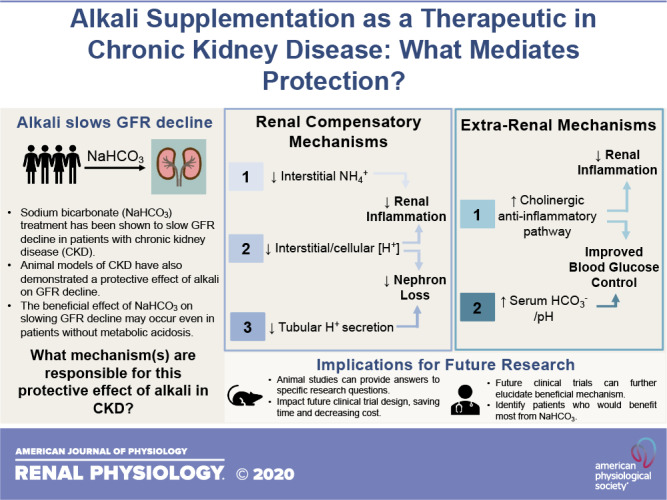
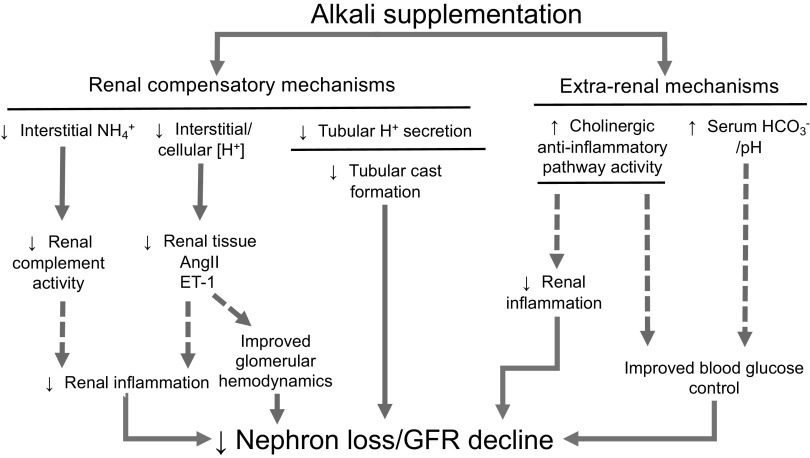
Sodium bicarbonate (NaHCO3) has been recognized as a possible therapy to target chronic kidney disease (CKD) progression. Several small clinical trials have demonstrated that supplementation with NaHCO3 or other alkalizing agents slows renal functional decline in patients with CKD. While the benefits of NaHCO3 treatment have been thought to result from restoring pH homeostasis, a number of studies have now indicated that NaHCO3 or other alkalis may provide benefit regardless of the presence of metabolic acidosis. These data have raised questions as to how NaHCO3 protects the kidneys. To date, the physiological mechanism(s) that mediates the reported protective effect of NaHCO3 in CKD remain unclear. In this review, we first examine the evidence from clinical trials in support of a beneficial effect of NaHCO3 and other alkali in slowing kidney disease progression and their relationship to acid-base status. Then, we discuss the physiological pathways that have been proposed to underlie these renoprotective effects and highlight strengths and weaknesses in the data supporting each pathway. Finally, we discuss how answering key questions regarding the physiological mechanism(s) mediating the beneficial actions of NaHCO3 therapy in CKD is likely to be important in the design of future clinical trials. We conclude that basic research in animal models is likely to be critical in identifying the physiological mechanisms underlying the benefits of NaHCO3 treatment in CKD. Gaining an understanding of these pathways may lead to the improved implementation of NaHCO3 as a therapy in CKD and perhaps other disease states.
Keywords: bicarbonate; blood glucose; cholinergic anti-inflammatory pathway; clinical trial; complement; glomerular filtration rate; metabolic acidosis; pH.
Conflict of interest statement
No conflicts of interest, financial or otherwise, are declared by the author(s).
Figures
References
-
- Adachi M, Hoshi M, Ushimaru S, Hayashi A, Nakamoto K, Kanbe A, Furuta N, Inagaki I, Ito H, Seishima M.. [Clinical significance of hyaline casts in the new CKD risk classification (KDIGO 2009)]. Rinsho Byori 61: 104−111, 2013. - PubMed
-
- Amdur RL, Feldman HI, Gupta J, Yang W, Kanetsky P, Shlipak M, Rahman M, Lash JP, Townsend RR, Ojo A, Roy-Chaudhury A, Go AS, Joffe M, He J, Balakrishnan VS, Kimmel PL, Kusek JW, Raj DS; CRIC Study Investigators . Inflammation and progression of CKD: the CRIC study. Clin J Am Soc Nephrol 11: 1546–1556, 2016. doi: 10.2215/CJN.13121215. - DOI - PMC - PubMed
-
- Banerjee T, Crews DC, Wesson DE, Tilea A, Saran R, Rios Burrows N, Williams DE, Powe NR; Centers for Disease Control and Prevention Chronic Kidney Disease Surveillance Team . Dietary acid load and chronic kidney disease among adults in the United States. BMC Nephrol 15: 137–137, 2014. doi: 10.1186/1471-2369-15-137. - DOI - PMC - PubMed
-
- Becker B, Kronenberg F, Kielstein JT, Haller H, Morath C, Ritz E, Fliser D; MMKD Study Group . Renal insulin resistance syndrome, adiponectin and cardiovascular events in patients with kidney disease: the mild and moderate kidney disease study. J Am Soc Nephrol 16: 1091–1098, 2005. doi: 10.1681/ASN.2004090742. - DOI - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical