

Geographic analysis of latent tuberculosis screening: A health system approach
- PMID: 33166372
- PMCID: PMC7652260
- DOI: 10.1371/journal.pone.0242055
Geographic analysis of latent tuberculosis screening: A health system approach
Abstract
Background: Novel approaches are required to better focus latent tuberculosis infection (LTBI) efforts in low-prevalence regions. Geographic information systems, used within large health systems, may provide one such approach.
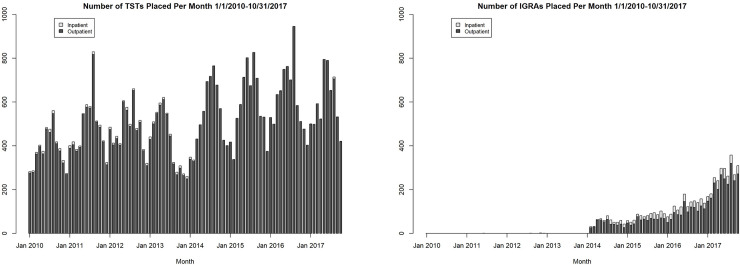
Methods: A retrospective, cross-sectional design was used to integrate US Census and Duke Health System data between January 1, 2010 and October 31, 2017 and examine the relationships between LTBI screening and population tuberculosis risk (assessed using the surrogate measure of proportion of persons born in tuberculosis-endemic regions) by census tract.
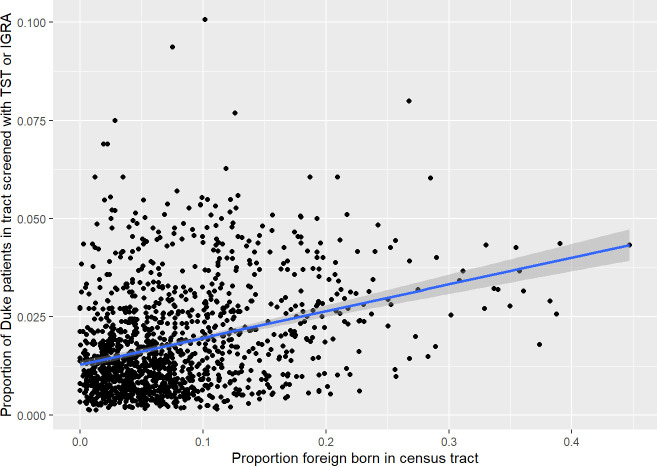
Results: The median proportion of Duke patients screened per census tract was 0.01 (range 0-0.1, interquartile range 0.01-0.03). The proportion of Duke patients screened within a census tract significantly but weakly correlated with the population risk. Furthermore, patients residing in census tracts with higher population tuberculosis risk were more likely to be screened with TST than with an IGRA (p<0.001).
Conclusion: The weak correlation between patient proportion screened for LTBI and our surrogate marker of population tuberculosis risk suggests that LTBI screening efforts should be better targeted. This type of geography-based analysis may serve as an easily obtainable benchmark for LTBI screening in health systems with low tuberculosis prevalence.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- Talwar A, Tsang C, Price S, Pratt R, Walker W, Schmit K, et al. Tuberculosis—United States, 2018. MMWR Morb Mortal Wkly Rep. 2018;68(11):257–62.
-
- Tasillo A, Salomon JA, Trikalinos TA, Horsburgh CR Jr., Marks SM, Linas BP. Cost-effectiveness of Testing and Treatment for Latent Tuberculosis Infection in Residents Born Outside the United States With and Without Medical Comorbidities in a Simulation Model. JAMA Intern Med. 2017;177(12):1755–64. - PMC - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
