

Stress CMR in patients with obesity: insights from the Stress CMR Perfusion Imaging in the United States (SPINS) registry
- PMID: 33166994
- PMCID: PMC8599869
- DOI: 10.1093/ehjci/jeaa281
Stress CMR in patients with obesity: insights from the Stress CMR Perfusion Imaging in the United States (SPINS) registry
Abstract
Aims: Non-invasive assessment and risk stratification of coronary artery disease in patients with large body habitus is challenging. We aim to examine whether body mass index (BMI) modifies the prognostic value and diagnostic utility of stress cardiac magnetic resonance imaging (CMR) in a multicentre registry.
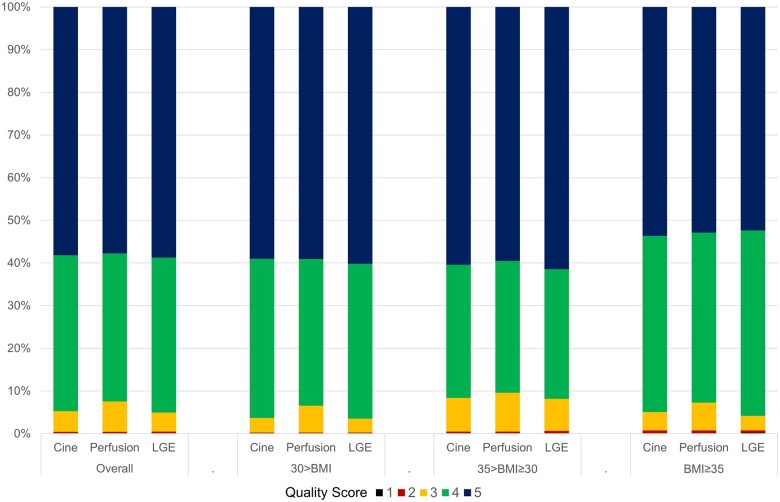
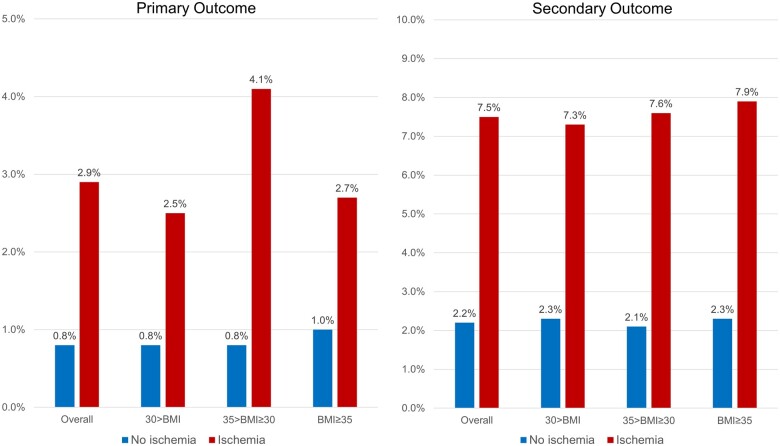
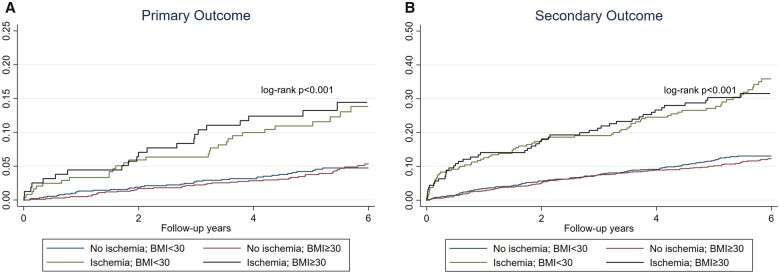
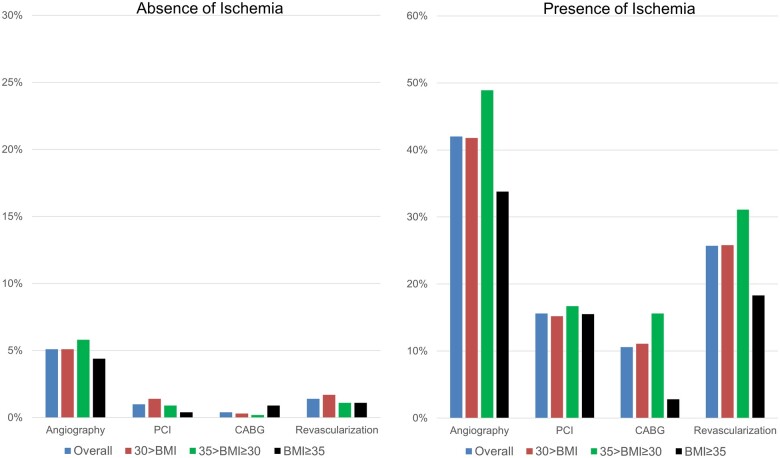
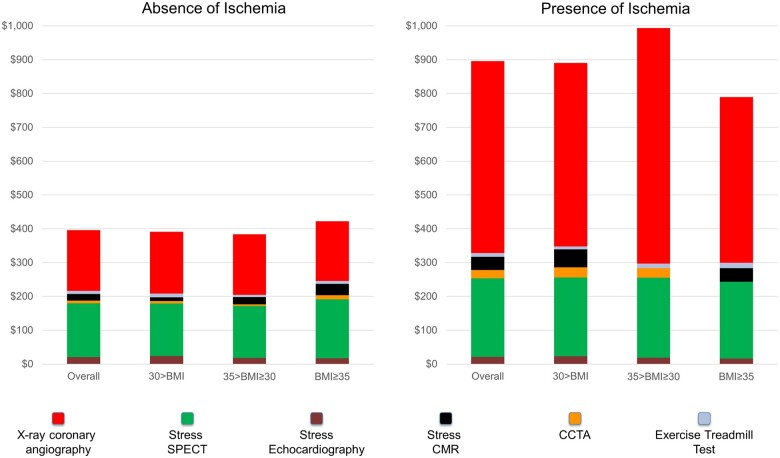
Methods and results: The SPINS Registry enrolled consecutive intermediate-risk patients who presented with a clinical indication for stress CMR in the USA between 2008 and 2013. Baseline demographic data including BMI, CMR indices, and ratings of study quality were collected. Primary outcome was defined by a composite of cardiovascular death and non-fatal myocardial infarction. Of the 2345 patients with available BMI included in the SPINS cohort, 1177 (50%) met criteria for obesity (BMI ≥ 30) with 531 (23%) at or above Class 2 obesity (BMI ≥ 35). In all BMI categories, >95% of studies were of diagnostic quality for cine, perfusion, and late gadolinium enhancement (LGE) sequences. At a median follow-up of 5.4 years, those without ischaemia and LGE experienced a low annual rate of hard events (<1%), across all BMI strata. In patients with obesity, both ischaemia [hazard ratio (HR): 2.14; 95% confidence interval (CI): 1.30-3.50; P = 0.003] and LGE (HR: 3.09; 95% CI: 1.83-5.22; P < 0.001) maintained strong adjusted association with the primary outcome in a multivariable Cox regression model. Downstream referral rates to coronary angiography, revascularization, and cost of care spent on ischaemia testing did not significantly differ within the BMI categories.
Conclusion: In this large multicentre registry, elevated BMI did not negatively impact the diagnostic quality and the effectiveness of risk stratification of patients referred for stress CMR.
Keywords: obesity; prognosis; stress cardiac MRI.
Published on behalf of the European Society of Cardiology. All rights reserved. © The Author(s) 2020. For permissions, please email: journals.permissions@oup.com.
Figures
Comment in
-
Cardiac magnetic resonance imaging: the echo of the obese?Eur Heart J Cardiovasc Imaging. 2021 Apr 28;22(5):528-529. doi: 10.1093/ehjci/jeaa327. Eur Heart J Cardiovasc Imaging. 2021. PMID: 33230522 No abstract available.
References
-
- Marques A, Peralta M, Naia A, Loureiro N, de Matos MG.. Prevalence of adult overweight and obesity in 20 European countries, 2014. Eur J Public Health 2018;28:295–300. - PubMed
-
- Mangold S, Wichmann JL, Schoepf UJ, Litwin SE, Canstein C, Varga-Szemes A. et al. Coronary CT angiography in obese patients using 3(rd) generation dual-source CT: effect of body mass index on image quality. Eur Radiol 2016;26:2937–46. - PubMed
-
- Leschka S, Stinn B, Schmid F, Schultes B, Thurnheer M, Baumueller S. et al. Dual source CT coronary angiography in severely obese patients: trading off temporal resolution and image noise. Invest Radiol 2009;44:720–7. - PubMed
-
- Ghanem MA, Kazim NA, Elgazzar AH.. Impact of obesity on nuclear medicine imaging. J Nucl Med Technol 2011;39:40–50. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
