

Rapid response to the alpha-1 adrenergic agent phenylephrine in the perioperative period is impacted by genomics and ancestry
- PMID: 33168928
- PMCID: PMC7997806
- DOI: 10.1038/s41397-020-00194-5
Rapid response to the alpha-1 adrenergic agent phenylephrine in the perioperative period is impacted by genomics and ancestry
Abstract
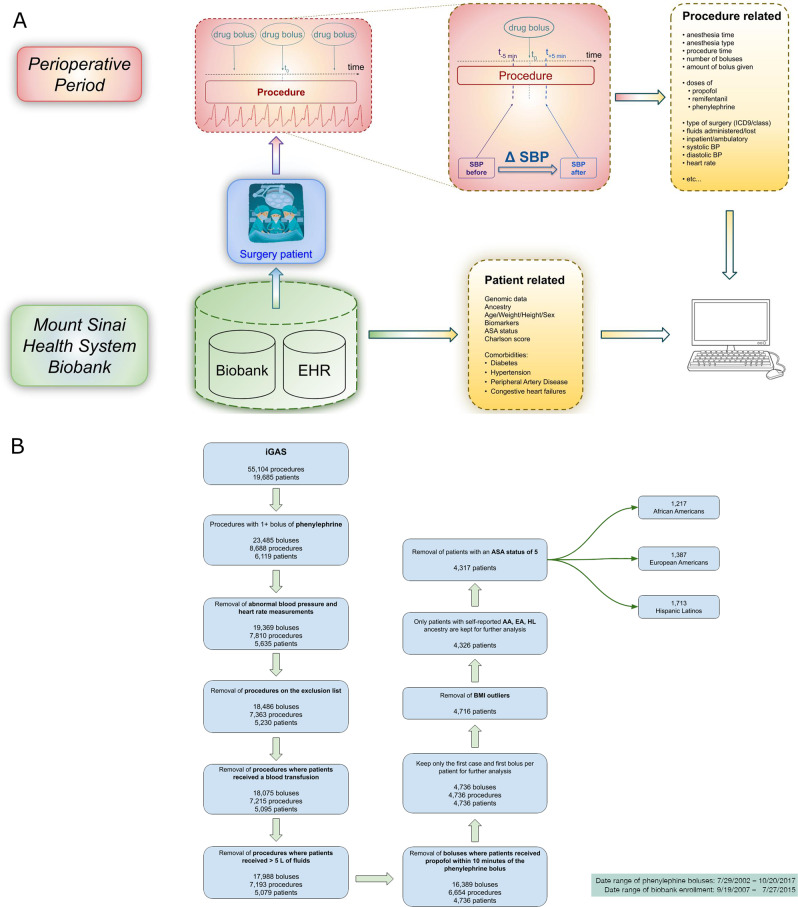
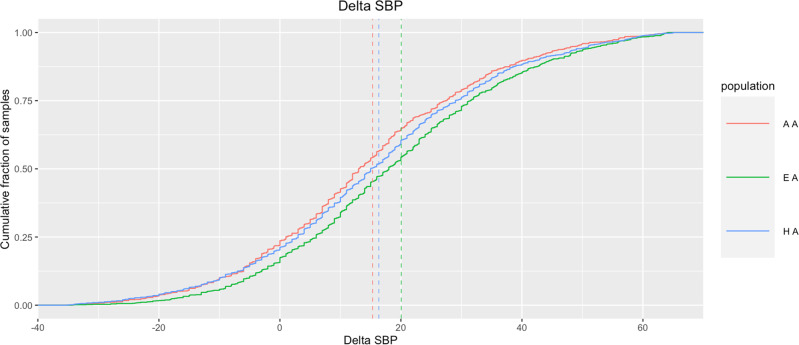
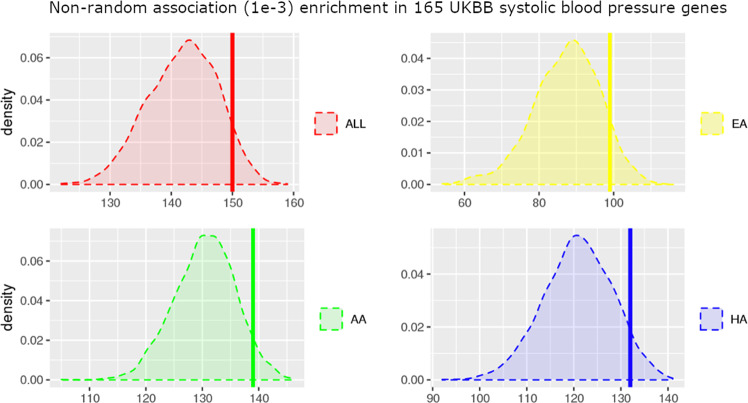
The emergence of genomic data in biobanks and health systems offers new ways to derive medically important phenotypes, including acute phenotypes occurring during inpatient clinical care. Here we study the genetic underpinnings of the rapid response to phenylephrine, an α1-adrenergic receptor agonist commonly used to treat hypotension during anesthesia and surgery. We quantified this response by extracting blood pressure (BP) measurements 5 min before and after the administration of phenylephrine. Based on this derived phenotype, we show that systematic differences exist between self-reported ancestry groups: European-Americans (EA; n = 1387) have a significantly higher systolic response to phenylephrine than African-Americans (AA; n = 1217) and Hispanic/Latinos (HA; n = 1713) (31.3% increase, p value < 6e-08 and 22.9% increase, p value < 5e-05 respectively), after adjusting for genetic ancestry, demographics, and relevant clinical covariates. We performed a genome-wide association study to investigate genetic factors underlying individual differences in this derived phenotype. We discovered genome-wide significant association signals in loci and genes previously associated with BP measured in ambulatory settings, and a general enrichment of association in these genes. Finally, we discovered two low frequency variants, present at ~1% in EAs and AAs, respectively, where patients carrying one copy of these variants show no phenylephrine response. This work demonstrates our ability to derive a quantitative phenotype suited for comparative statistics and genome-wide association studies from dense clinical and physiological measures captured for managing patients during surgery. We identify genetic variants underlying non response to phenylephrine, with implications for preemptive pharmacogenomic screening to improve safety during surgery.
Conflict of interest statement
EEK has received speaker honorariums from Illumina, Inc and Regeneron, Inc.
Figures


References
-
- Bijker JB, van Klei WA, Vergouwe Y, Eleveld DJ, van Wolfswinkel L, Moons KGM, et al. Intraoperative hypotension and 1-year mortality after noncardiac surgery. Anesthesiology. 2009;111:1217–26. - PubMed
-
- Levin MA, Fischer GW, Lin H-M, McCormick PJ, Krol M, Reich DL. Intraoperative arterial blood pressure lability is associated with improved 30 day survival. Br J Anaesth. 2015;115:716–26. - PubMed
-
- Monk TG, Saini V, Weldon BC, Sigl JC. Anesthetic management and one-year mortality after noncardiac surgery. Anesth Analg. 2005;100:4–10. - PubMed
-
- Sessler DI, Sigl JC, Kelley SD, Chamoun NG, Manberg PJ, Saager L, et al. Hospital stay and mortality are increased in patients having a ‘triple low’ of low blood pressure, low bispectral index, and low minimum alveolar concentration of volatile anesthesia. Anesthesiology. 2012;116:1195–203. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
