

How to ventilate obstructive and asthmatic patients
- PMID: 33169215
- PMCID: PMC7652057
- DOI: 10.1007/s00134-020-06291-0
How to ventilate obstructive and asthmatic patients
Abstract
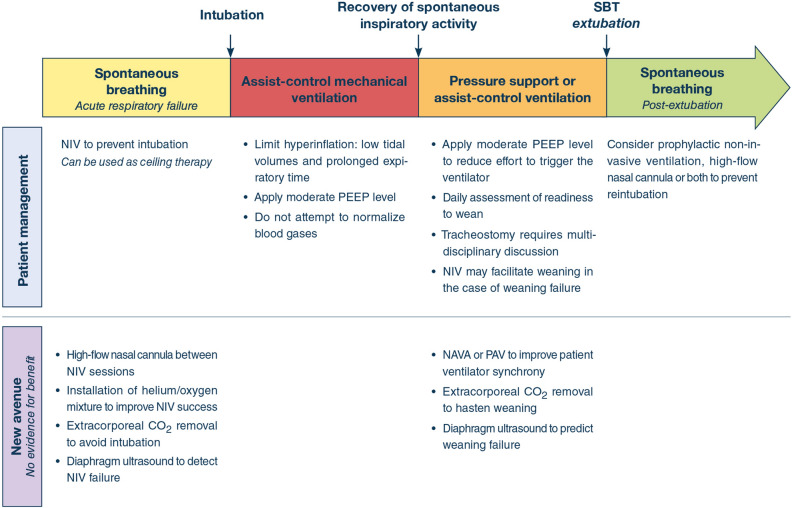
Exacerbations are part of the natural history of chronic obstructive pulmonary disease and asthma. Severe exacerbations can cause acute respiratory failure, which may ultimately require mechanical ventilation. This review summarizes practical ventilator strategies for the management of patients with obstructive airway disease. Such strategies include non-invasive mechanical ventilation to prevent intubation, invasive mechanical ventilation, from the time of intubation to weaning, and strategies intended to prevent post-extubation acute respiratory failure. The role of tracheostomy, the long-term prognosis, and potential future adjunctive strategies are also discussed. Finally, the physiological background that underlies these strategies is detailed.
Keywords: Asthma; Chronic obstructive pulmonary disease; Intrisic positive end-expiratory pressure (PEEP); Mechanical ventilation; Non-invasive ventilation; Weaning.
Conflict of interest statement
AD reports personal fees from Medtronic, grants, personal fees and non-financial support from Philips, personal fees from Baxter, personal fees from Hamilton, personal fees and non-financial support from Fisher & Paykel, grants from French Ministry of Health, personal fees from Getinge, grants and personal fees from Respinor, grants and non-financial support from Lungpacer, outside the submitted work. LB conducts an investigator-initiated trial on PAV+ (NCT02447692) funded by the Canadian Institute for Health Research and a partnership with Medtronic Covidien; his laboratory also receives grants and non-financial support from Fisher & Paykel, non-financial support from Air Liquide Medical System, non-financial support from Philips, non-financial support from Sentec, other from General Electric (patent). MD reports personal fees from Lungpacer Med Inc, grants from French Ministry of Heath outside the submitted work. LH reports a research grant paid to institution from Liberate Medical (USA) and speakers fee from Getinge Critical Care. AJ reports grant from the National Institute of Health (RO1-NR016055). FL reports research grants from the National Institutes of Health, VA Research Service, Liberate Medical LLC, and the National Science Foundation, all outside the submitted work. AM-D reports research grants from Fischer Paykel, Baxter, Philips, Ferring and GSK; participation to advisory board for Air Liquide, Baxter, and Amomed, lectures for Getingue and Addmedica. SN report advisory board for Philips and Breas and speaking fee from Resmed Italy outside the submitted work. OP reports no conflict of interest. LO-B reports no conflict of interest. LP reports lecture fees from Hamilton Medical and Getinge and personal fees from Löwenstein, all outside the submitted work. TV reports no conflict of interest. JM reports personal fees from Faron, personal fees from Medtronic, personal fees from Janssen, grants from Covidien (Medtronic) and CIHR, and reimboursement of travel and hotel expenses to attend a meeting from IMT Medical, all outside the submitted work.
Figures





References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
