

Admission Cardiac Diagnostic Testing with Electrocardiography and Troponin Measurement Prognosticates Increased 30-Day Mortality in COVID-19
- PMID: 33169643
- PMCID: PMC7955502
- DOI: 10.1161/JAHA.120.018476
Admission Cardiac Diagnostic Testing with Electrocardiography and Troponin Measurement Prognosticates Increased 30-Day Mortality in COVID-19
Abstract
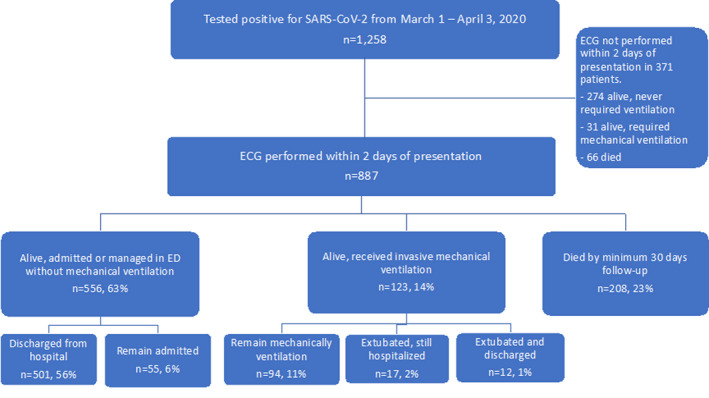
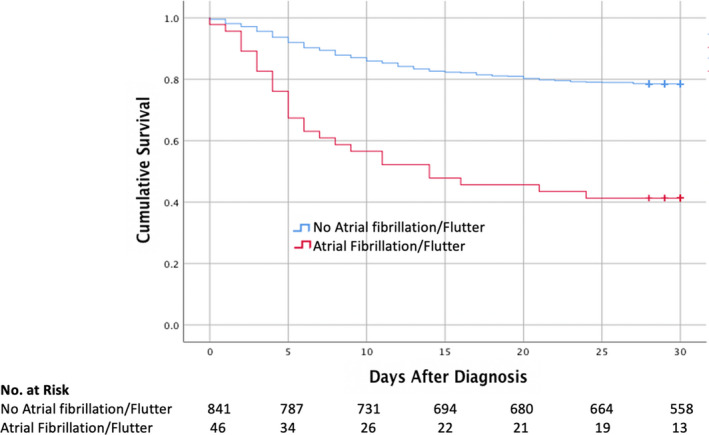
Background Cardiovascular involvement in coronavirus disease 2019 (COVID-19) is common and leads to worsened mortality. Diagnostic cardiovascular studies may be helpful for resource appropriation and identifying patients at increased risk for death. Methods and Results We analyzed 887 patients (aged 64±17 years) admitted with COVID-19 from March 1 to April 3, 2020 in New York City with 12 lead electrocardiography within 2 days of diagnosis. Demographics, comorbidities, and laboratory testing, including high sensitivity cardiac troponin T (hs-cTnT), were abstracted. At 30 days follow-up, 556 patients (63%) were living without requiring mechanical ventilation, 123 (14%) were living and required mechanical ventilation, and 203 (23%) had expired. Electrocardiography findings included atrial fibrillation or atrial flutter (AF/AFL) in 46 (5%) and ST-T wave changes in 306 (38%). 27 (59%) patients with AF/AFL expired as compared to 181 (21%) of 841 with other non-life-threatening rhythms (P<0.001). Multivariable analysis incorporating age, comorbidities, AF/AFL, QRS abnormalities, and ST-T wave changes, and initial hs-cTnT ≥20 ng/L showed that increased age (HR 1.04/year), elevated hs-cTnT (HR 4.57), AF/AFL (HR 2.07), and a history of coronary artery disease (HR 1.56) and active cancer (HR 1.87) were associated with increased mortality. Conclusions Myocardial injury with hs-cTnT ≥20 ng/L, in addition to cardiac conduction perturbations, especially AF/AFL, upon hospital admission for COVID-19 infection is associated with markedly increased risk for mortality than either diagnostic abnormality alone.
Keywords: COVID‐19; arrhythmia; atrial fibrillation; troponin.
Conflict of interest statement
TJP owns stock in Abbott Laboratories, AbbVie, Inc, Baxter International, and Edwards Lifesciences, has received research funding from the Amyloidosis Foundation David Seldin Memorial Junior Research Grant, and has research grant funding pending from EIDOS Therapeutic, which is unrelated to this research.
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
