

Recognizing Cardiovascular Risk After Preeclampsia: The P4 Study
- PMID: 33170079
- PMCID: PMC7763721
- DOI: 10.1161/JAHA.120.018604
Recognizing Cardiovascular Risk After Preeclampsia: The P4 Study
Abstract
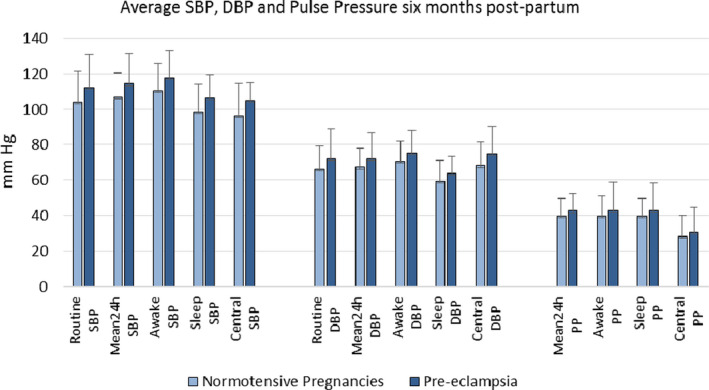
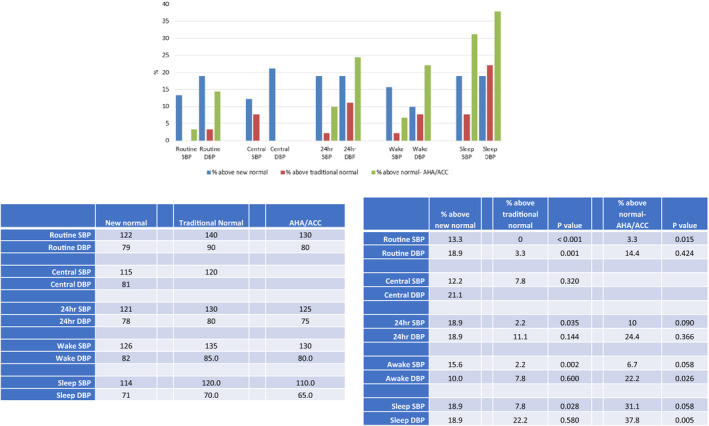
Background There is increased risk of hypertension, early cardiovascular disease, and premature mortality in women who have had preeclampsia. This study was undertaken to determine the upper limit of normal blood pressure (BP) 6 months postpartum and the frequency of women with prior preeclampsia who had BP above these limits, as part of the P4 (Post-Partum Physiology, Psychology and Pediatric) follow-up study. Methods and Results BP was measured by sphygmomanometer, 24-hour ambulatory BP monitoring, and non-invasive central BP at 6 months postpartum in 302 women who had normotensive pregnancy and 90 who had preeclampsia. The upper limit of normal BP (mean+2 SD) for women with normotensive pregnancy was 122/79 mm Hg for routine BP, 115/81 mm Hg for central BP, and 121/78 mm Hg for 24-hour ambulatory BP monitoring. Traditional normal values detected only 3% of women who had preeclampsia as having high BP 6 months postpartum whereas these new values detected between 13% and 19%. Women with preeclampsia had greater body mass index (27.8 versus 25.0, P<0.001) and left ventricular wall thickness but similar augmentation index. They also had lower high-density lipoprotein (59±15 versus 65±16 mg/dL, P=0.002), higher triglycerides (77±51 versus 61±35 mg/dL, P=0.005), and higher homeostatic model assessment score (2.1±1.8 versus 1.3±1.9, P<0.001). Conclusions Clinicians wishing to detect high BP in these women should be aware of the lower than usual upper limit of normal for this young cohort and where possible should use 24-hour ambulatory BP monitoring to detect these changes. This may define a subgroup of women who had preeclampsia for whom targeted BP lowering therapy would be successful. Registration URL: https://anzctr.org.au/Trial/Registration/TrialReview.aspx?id=365295&isReview=true; Unique identifier: ACTRN12613001260718.
Keywords: blood pressure monitoring; cardiovascular risk; high blood pressure; preeclampsia; pregnancy hypertension.
Conflict of interest statement
None.
Figures
References
-
- Leon LJ, McCarthy FP, Direk K, Gonzalez‐Izquierdo A, Prieto‐Merino D, Casas JP, Chappell L. Preeclampsia and cardiovascular disease in a large UK pregnancy cohort of linked electronic health records. Circulation. 2019;140:1050–1060. - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
