

Treatment of intraoperative hypotension with cafedrine/theodrenaline versus ephedrine : A prospective, national, multicenter, non-interventional study-the HYPOTENS trial
- PMID: 33170310
- PMCID: PMC8026467
- DOI: 10.1007/s00101-020-00877-5
Treatment of intraoperative hypotension with cafedrine/theodrenaline versus ephedrine : A prospective, national, multicenter, non-interventional study-the HYPOTENS trial
Erratum in
-
[Erratum to: Treatment of intraoperative hypotension with cafedrine/theodrenaline versus ephedrine. A prospective, national, multicenter, non-interventional study-the HYPOTENS trial].Anaesthesist. 2021 Apr;70(4):358. doi: 10.1007/s00101-021-00932-9. Anaesthesist. 2021. PMID: 33635373 Free PMC article. German. No abstract available.
Abstract
Background: Sympathomimetic drugs are a therapeutic cornerstone for the management of hypotensive states like intraoperative hypotension (IOH). While cafedrine/theodrenaline (C/T) is widely used in Germany to restore blood pressure in patients with IOH, more research is required to compare its effectiveness with alternatives such as ephedrine (E) that are more commonly available internationally.
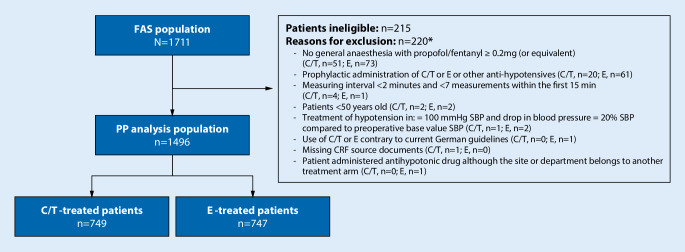
Methods: HYPOTENS (NCT02893241, DRKS00010740) was a prospective, national, multicenter, open-label, two-armed, non-interventional study that compared C/T with E for treatment of IOH. We describe a prospectively defined cohort of patients ≥50 years old with comorbidities undergoing general anesthesia induced with propofol and fentanyl. Primary objectives were to examine treatment precision, rapidity of onset and the ability to restore blood pressure without relevant increases in heart rate. Secondary endpoints were treatment satisfaction and the number of required additional boluses or other accompanying measures.
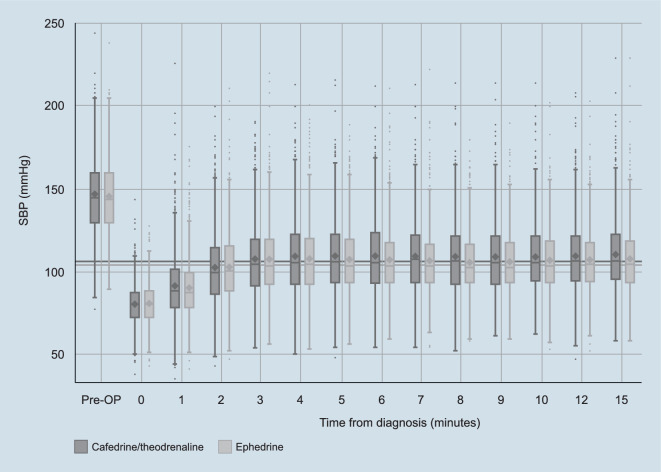
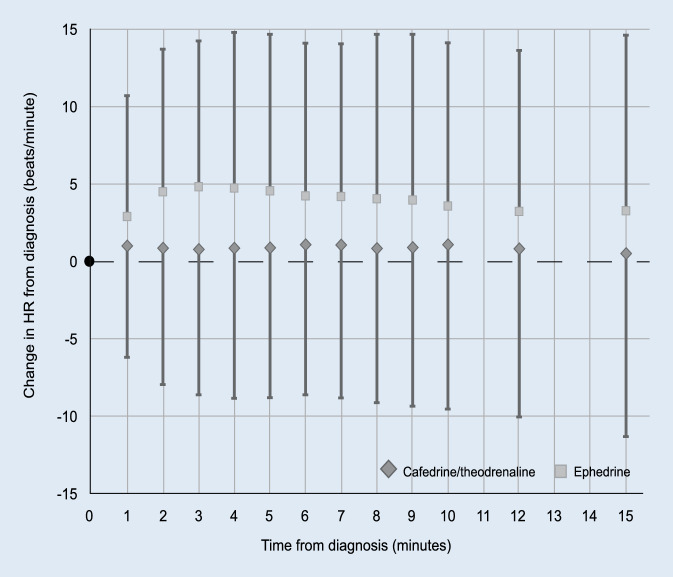
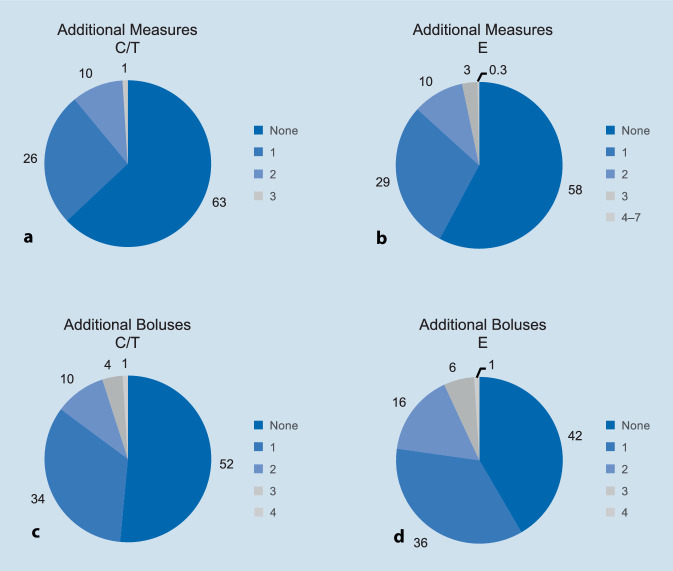
Results: A total of 1496 patients were included in the per protocol analysis. Overall, effective stabilization of blood pressure was achieved with both C/T and E. Post-hoc analysis showed that blood pressure increase from baseline was more pronounced with C/T. Fewer additional boluses or other accompanying measures were required in the C/T arm. The incidence of tachycardia was comparable between groups. Post-hoc analysis showed that E produced dose-dependent elevated heart rate values. By contrast, heart rate remained stable in patients treated with C/T. Physicians reported a higher level of treatment satisfaction with C/T, with a higher proportion of anesthetists rating treatment precision and rapidity of onset as good or very good when compared with E.
Conclusion: Neither drug was superior in restoring blood pressure levels; however, post-hoc analyses suggested that treatment is more goal-orientated and easier to control with C/T. Heart rate was shown to be more stable with C/T and fewer additional interventions were required to restore blood pressure, which could have contributed to the increased treatment satisfaction reported by anesthetists using C/T.
Zusammenfassung: HINTERGRUND: Die medikamentöse Therapie mit Sympathomimetika bildet einen Grundpfeiler der Behandlung relevanter Blutdruckabfälle, so auch der intraoperativen Hypotonie (IOH). Dieses häufige Problem ist mit Endorganschäden assoziiert, wobei Nierenversagen und eine erhöhte Rate kardiovaskulärer Komplikationen am besten dokumentiert sind. Die Datenlage verdeutlicht die Notwendigkeit, dass eine IOH schnell und konsequent therapiert werden muss. Obwohl Cafedrin/Theodrenalin (C/T) in Deutschland häufig in dieser Indikation eingesetzt wird, fehlte bislang ein Wirksamkeitsvergleich mit international verfügbaren Alternativen wie Ephedrin (E).
Methoden: HYPOTENS ist eine prospektive, nationale, multizentrische (53 Kliniken mit 66 operativen Abteilungen), offene, zweiarmige, nicht-interventionelle Studie zum Vergleich der Wirksamkeit von C/T und E bei der IOH-Therapie unter klinischen Routinebedingungen. Diese Studie beschreibt eine prospektiv definierte Kohorte von Patienten im Alter von ≥50 Jahren mit Komorbiditäten, deren Allgemeinanästhesie mit Propofol und Fentanyl (≥0,2 mg oder Äquivalent) eingeleitet wurde. Alle Patienten hatten intraoperativ eine therapiepflichtige IOH entwickelt und wurden nach dem jeweiligen lokalen Standard mit C/T oder E therapiert. Die primären Studienziele waren Präzision und Schnelligkeit des Blutdruckanstiegs auf einen vor der Behandlung individuell festgelegten Mindest-Zielblutdruck, ohne dabei einen relevanten Anstieg der Herzfrequenz zu verursachen. Die Therapiezufriedenheit der Anästhesisten und die Anzahl zusätzlicher Bolusinjektionen oder weiterer kreislaufstabilisierender Maßnahmen waren sekundäre Endpunkte.
Ergebnisse: Insgesamt 1496 Patienten wurden protokollgemäß behandelt und ausgewertet. Eine Kreislaufstabilisierung wurde mit beiden Therapieoptionen erreicht. Post-hoc-Analysen zeigen, dass der Blutdruckanstieg unter C/T ausgeprägter war und gleichzeitig weniger zusätzliche Boli der jeweiligen Substanz appliziert und zusätzliche kreislaufstabilisierende Interventionen durchgeführt werden mussten. Die Inzidenz von Tachykardien war in beiden Behandlungsgruppen vergleichbar. Unter E kam es jedoch zu einer dosisabhängigen Erhöhung der Herzfrequenz, während bei den mit C/T behandelten Patienten die Herzfrequenz stabil blieb. Die Therapiezufriedenheit der Anästhesisten war im C/T-Arm höher.
Schlussfolgerung: Hinsichtlich der Kreislaufstabilisierung war keine der beiden Therapieoptionen überlegen. Post-hoc-Analysen deuten darauf hin, dass C/T unter Routinebedingungen eine zielorientiertere und einfacher zu steuernde Kreislaufstabilisierung ermöglicht. Die seltener erforderlichen erweiterten Therapiemaßnahmen zur ergänzenden IOH-Korrektur stellen einen möglichen Grund für die höhere Anwenderzufriedenheit dar.
Keywords: Akrinor; Cafedrine, theodrenaline drug combination; Catecholamines; Ephedrine; Haemodynamics; Hypotension; Sympathomimetics; Vasopressor.
Conflict of interest statement
L. Eberhart has received consultant and lecture fees from ratiopharm GmbH (part of the Teva Group) and supports ongoing research by ratiopharm. G. Geldner and T. Koch have received consulting fees from ratiopharm GmbH and support ongoing research by ratiopharm. S. Huljic is an employee of ratiopharm GmbH. T. Keller and S. Weber were subcontractors of the contract research organization commissioned by the study sponsor (Mediveritas GmbH, Munich). P. Kranke has received lecturing fees from ratiopharm GmbH (part of the Teva Group) as well as from Sintetica and supports ongoing research from ratiopharm. All study centers received compensation for each recruited and documented patient (€ 150 per case). All remaining authors (A. Kowark, T.-P. Zucker, S. Kreuer and M. Przemeck) declare no other conflicts of interest.
Figures
References
-
- Ratiopharm (2016) Akrinor® prescribing information. https://www.ratiopharm.de/assets/products/de/label/Akrinor%C2%AE%20200%2.... Accessed 30 Apr 2020
-
- Sintetica (2017) Ephedrine meduna prescribing information. https://sintetica.de/wp-content/uploads/2019/08/FI-Ephedrin-Meduna-10mgm.... Accessed 30 Apr 2020
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
