

Analgesia and sedation in patients with ARDS
- PMID: 33170331
- PMCID: PMC7653978
- DOI: 10.1007/s00134-020-06307-9
Analgesia and sedation in patients with ARDS
Abstract
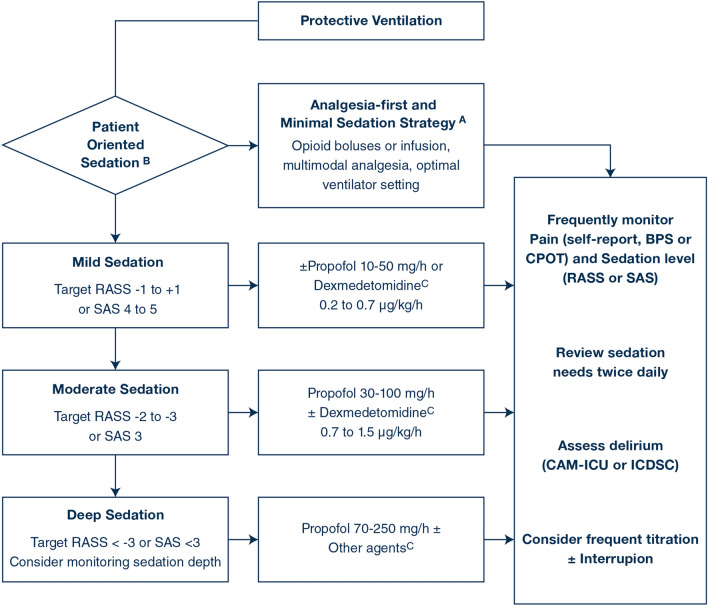
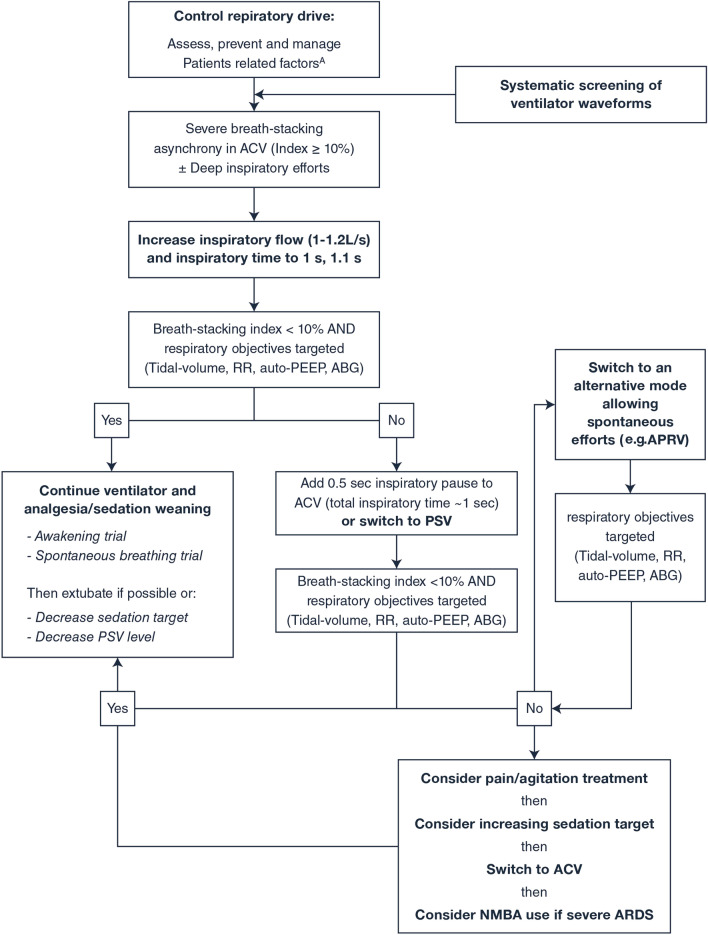
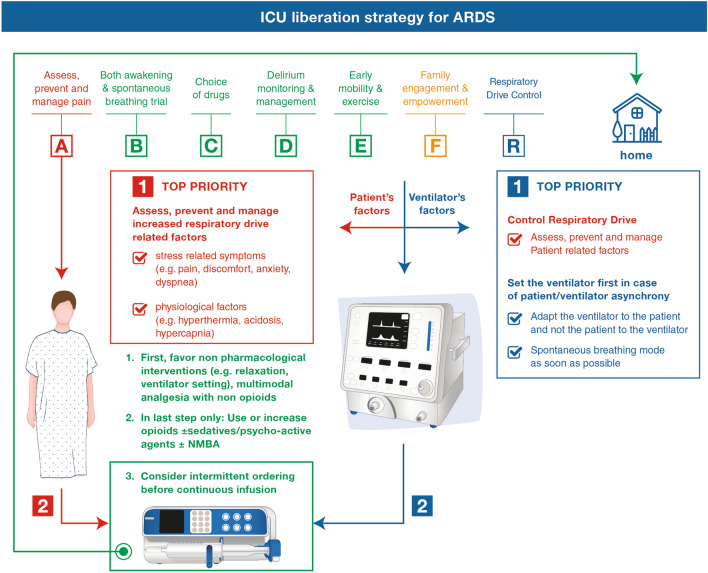
Acute Respiratory Distress Syndrome (ARDS) is one of the most demanding conditions in an Intensive Care Unit (ICU). Management of analgesia and sedation in ARDS is particularly challenging. An expert panel was convened to produce a "state-of-the-art" article to support clinicians in the optimal management of analgesia/sedation in mechanically ventilated adults with ARDS, including those with COVID-19. Current ICU analgesia/sedation guidelines promote analgesia first and minimization of sedation, wakefulness, delirium prevention and early rehabilitation to facilitate ventilator and ICU liberation. However, these strategies cannot always be applied to patients with ARDS who sometimes require deep sedation and/or paralysis. Patients with severe ARDS may be under-represented in analgesia/sedation studies and currently recommended strategies may not be feasible. With lightened sedation, distress-related symptoms (e.g., pain and discomfort, anxiety, dyspnea) and patient-ventilator asynchrony should be systematically assessed and managed through interprofessional collaboration, prioritizing analgesia and anxiolysis. Adaptation of ventilator settings (e.g., use of a pressure-set mode, spontaneous breathing, sensitive inspiratory trigger) should be systematically considered before additional medications are administered. Managing the mechanical ventilator is of paramount importance to avoid the unnecessary use of deep sedation and/or paralysis. Therefore, applying an "ABCDEF-R" bundle (R = Respiratory-drive-control) may be beneficial in ARDS patients. Further studies are needed, especially regarding the use and long-term effects of fast-offset drugs (e.g., remifentanil, volatile anesthetics) and the electrophysiological assessment of analgesia/sedation (e.g., electroencephalogram devices, heart-rate variability, and video pupillometry). This review is particularly relevant during the COVID-19 pandemic given drug shortages and limited ICU-bed capacity.
Keywords: Acute respiratory distress syndrome; Analgesia; COVID-19; Intensive care unit; Mechanical ventilation; Rehabilitation; Sedation.
Conflict of interest statement
GC declares fees for speaker (Orion pharma, Aspen medical) and participation to scientific board (Orion pharma); J-MC declares fees for speaker (Orion pharma, Baxter, Sedana Medical) and participation to scientific board (Orion pharma, Baxter, Sedana Medical); TG declares participation in a scientific board (Haisco Pharmaceutical); Matthieu Jabaudon reports research grants and fees for participation to an advisory board from Sedana Medical, and fees and non-financial support for a seminar from GE Healthcare; SJ reports consulting fees from Drager, Xenios, Medtronic and Fisher and Paykel; PP reports a research grant from Pfizer in collaboration with the NIH; J-FP declares fees for speaker and participation to scientific board (Orion pharma); YS and/or his institution received grants from the Australian National Health and Medical Research Council, research grants and in-kind support for the SPICE III trial from Pfizer and Orion Pharma and speaker’s honorarium for participation in educational events from Pfizer, Orion Pharma and Abbott laboratories; JWD, EWE, GLF, CG, CG, JPK, TL, SM, MJM, BP, KP, BR, TS and HTO declare no conflict of interest.
Figures
References
-
- Bellani G, Laffey JG, Pham T, Fan E, Brochard L, Esteban A, Gattinoni L, van Haren F, Larsson A, McAuley DF, Ranieri M, Rubenfeld G, Thompson BT, Wrigge H, Slutsky AS, Pesenti A. Epidemiology, patterns of care, and mortality for patients with acute respiratory distress syndrome in intensive care units in 50 countries. JAMA. 2016;315:788–800. - PubMed
-
- Devlin JW, Skrobik Y, Gelinas C, Needham DM, Slooter AJC, Pandharipande PP, Watson PL, Weinhouse GL, Nunnally ME, Rochwerg B, Balas MC, van den Boogaard M, Bosma KJ, Brummel NE, Chanques G, Denehy L, Drouot X, Fraser GL, Harris JE, Joffe AM, Kho ME, Kress JP, Lanphere JA, McKinley S, Neufeld KJ, Pisani MA, Payen JF, Pun BT, Puntillo KA, Riker RR, Robinson BRH, Shehabi Y, Szumita PM, Winkelman C, Centofanti JE, Price C, Nikayin S, Misak CJ, Flood PD, Kiedrowski K, Alhazzani W. Clinical practice guidelines for the prevention and management of pain, agitation/sedation, delirium, immobility, and sleep disruption in adult patients in the ICU. Crit Care Med. 2018;46:e825–e873. - PubMed
-
- Chanques G, Drouot X, Payen JF. 2008–2018: ten years of gradual changes in the sedation guidelines for critically ill patients. Anaesth Crit Care Pain Med. 2018;37:509–511. - PubMed
-
- Papazian L, Forel JM, Gacouin A, Penot-Ragon C, Perrin G, Loundou A, Jaber S, Arnal JM, Perez D, Seghboyan JM, Constantin JM, Courant P, Lefrant JY, Guerin C, Prat G, Morange S, Roch A, Investigators AS. Neuromuscular blockers in early acute respiratory distress syndrome. N Engl J Med. 2010;363:1107–1116. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
