

Robotic rectal resection: oncologic outcomes
- PMID: 33170489
- PMCID: PMC8184562
- DOI: 10.1007/s13304-020-00911-6
Robotic rectal resection: oncologic outcomes
Abstract
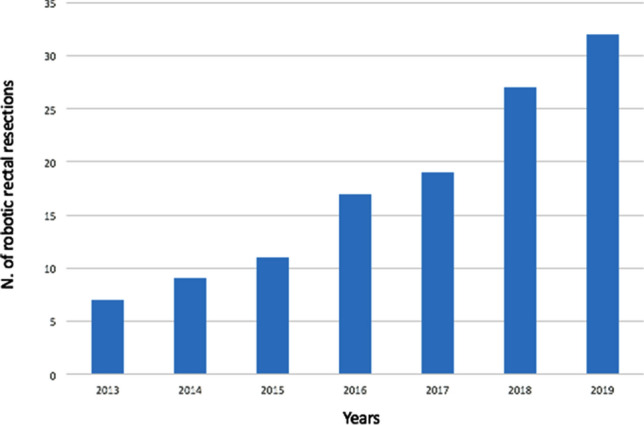
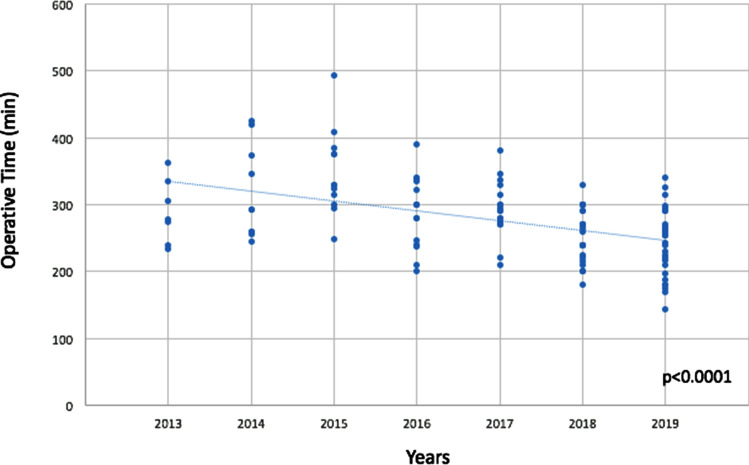
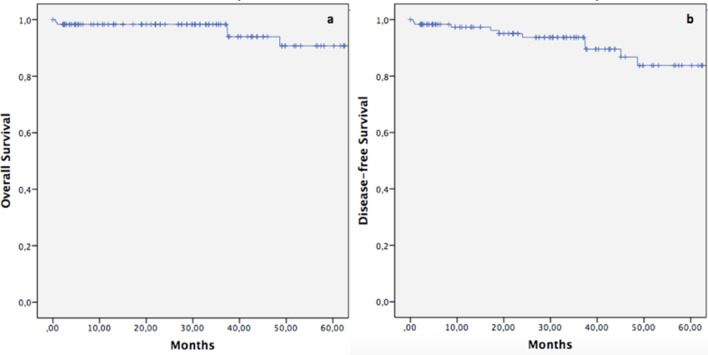
Robotic surgery has progressively gained popularity in the treatment of rectal cancer. However, only a few studies on its oncologic effectiveness are currently present, with contrasting results. The purpose of this study is to report a single surgeon's experience on robotic rectal resection (RRR) for cancer, focusing on the analysis of oncologic outcomes, both in terms of pathological features and long-term results. One-hundred and twenty-two consecutive patients who underwent RRR for rectal cancer from January 2013 to December 2019 were retrospectively enrolled. Patients' characteristics and perioperative outcomes were collected. The analyzed oncologic outcomes were pathological features [distal (DM), circumferential margin (CRM) status and quality of mesorectal excision (TME)] and long-term outcomes [overall (OS) and disease-free survival (DFS)]. The mean operative time was 275 (± 60.5) minutes. Conversion rate was 6.6%. Complications occurred in 27 cases (22.1%) and reoperation was needed in 2 patients (1.5%). The median follow-up was 30.5 (5.9-86.1) months. None presented DM positivity. CRM positivity was 2.5% (2 cases) while a complete TME was reached in 94.3% of cases (115 patients). Recurrence rate was 5.7% (2 local, 4 distant and 1 local plus distant tumor relapse). OS and DFS were 90.7% and 83%, respectively. At the multivariate analysis, both CRM positivity and near complete/incomplete TME were recognized as negative prognostic factors for OS and DFS. Under appropriate logistic and operative conditions, robotic surgery for rectal cancer proves to be oncologically effective, with adequate pathological results and long-term outcomes. It also offers acceptable peri-operative outcomes, further confirming the safety and feasibility of the technique.
Keywords: Long-term outcomes; Oncological outcomes; Rectal cancer; Robotic surgery.
Conflict of interest statement
authors declare that they have no conflict of interest.
Figures
References
-
- Kim J, Baek S-J, Kang D-W, Roh Y-E, Lee JW, Kwak H-D, Kwak JM, Kim S-H. Robotic resection is a good prognostic factor in rectal cancer compared with laparoscopic resection: long-term survival analysis using propensity score matching. Dis Colon Rectum. 2017;60(3):266–273. doi: 10.1097/DCR.0000000000000770. - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
