

What matters most: Randomized controlled trial of breast cancer surgery conversation aids across socioeconomic strata
- PMID: 33170506
- PMCID: PMC7983934
- DOI: 10.1002/cncr.33248
What matters most: Randomized controlled trial of breast cancer surgery conversation aids across socioeconomic strata
Abstract
Background: Women of lower socioeconomic status (SES) with early-stage breast cancer are more likely to report poorer physician-patient communication, lower satisfaction with surgery, lower involvement in decision making, and higher decision regret compared to women of higher SES. The objective of this study was to understand how to support women across socioeconomic strata in making breast cancer surgery choices.
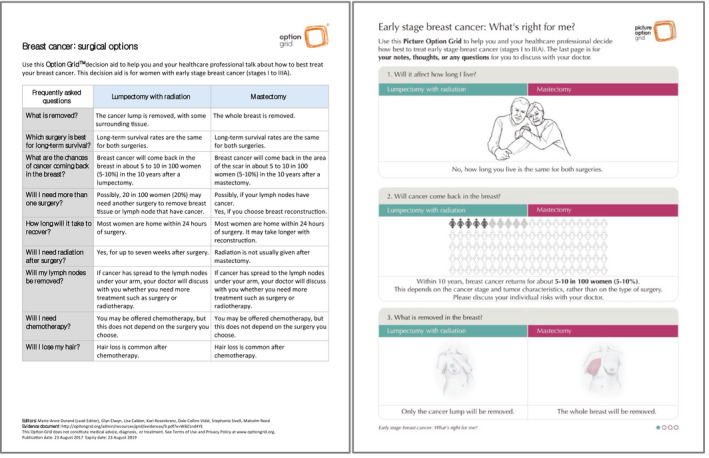
Methods: We conducted a 3-arm (Option Grid, Picture Option Grid, and usual care), multisite, randomized controlled superiority trial with surgeon-level randomization. The Option Grid (text only) and Picture Option Grid (pictures plus text) conversation aids were evidence-based summaries of available breast cancer surgery options on paper. Decision quality (primary outcome), treatment choice, treatment intention, shared decision making (SDM), anxiety, quality of life, decision regret, and coordination of care were measured from T0 (pre-consultation) to T5 (1-year after surgery.
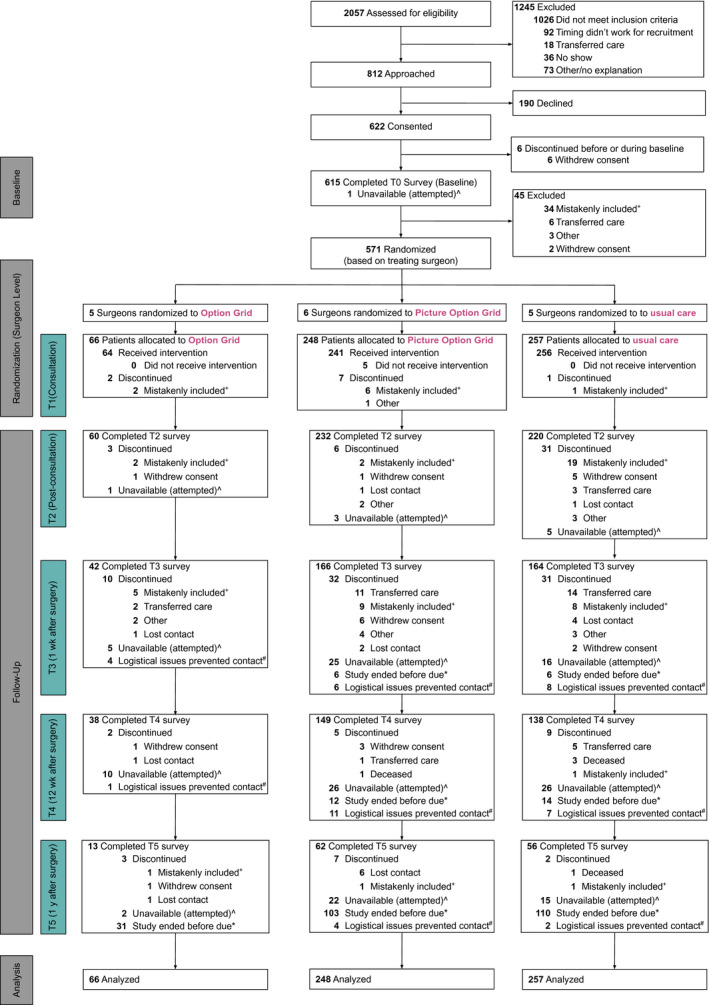
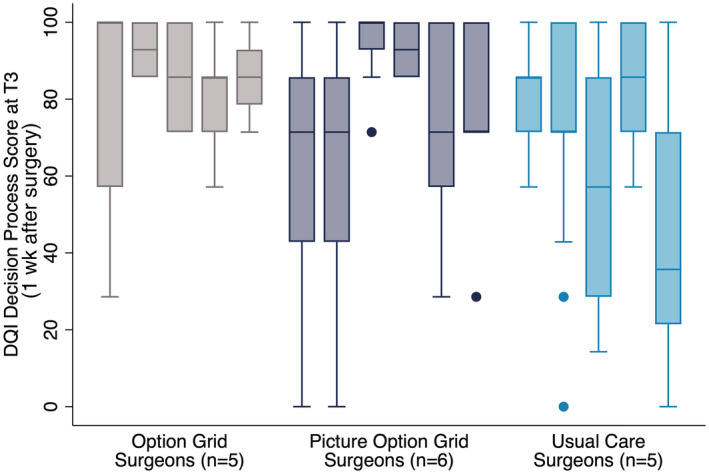
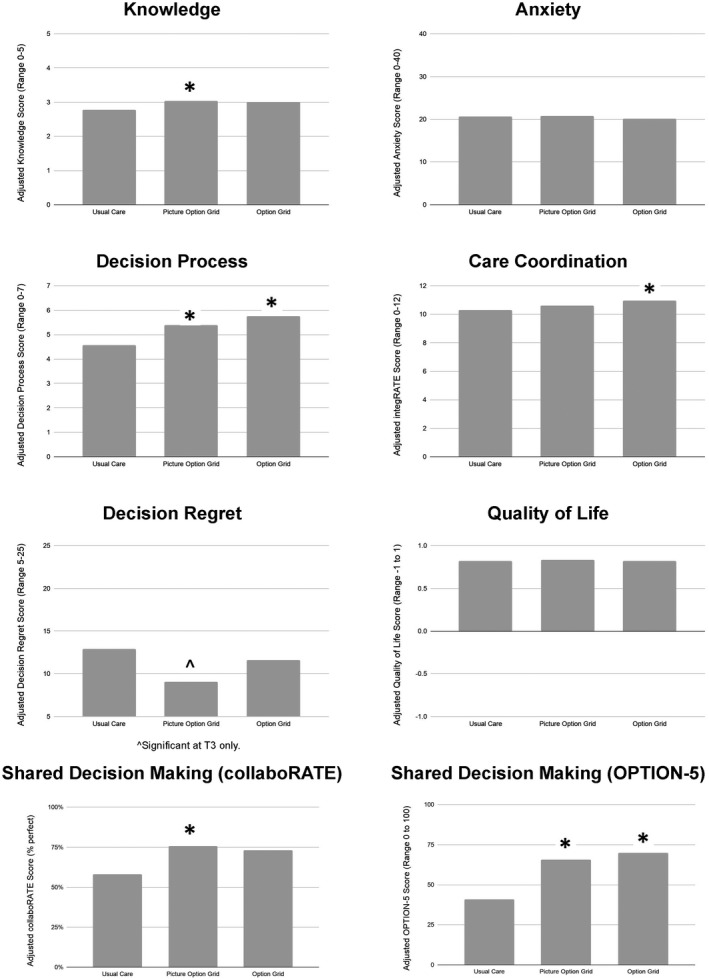
Results: Sixteen surgeons saw 571 of 622 consented patients. Patients in the Picture Option Grid arm (n = 248) had higher knowledge (immediately after the visit [T2] and 1 week after surgery or within 2 weeks of the first postoperative visit [T3]), an improved decision process (T2 and T3), lower decision regret (T3), and more SDM (observed and self-reported) compared to usual care (n = 257). Patients in the Option Grid arm (n = 66) had higher decision process scores (T2 and T3), better coordination of care (12 weeks after surgery or within 2 weeks of the second postoperative visit [T4]), and more observed SDM (during the surgical visit [T1]) compared to usual care arm. Subgroup analyses suggested that the Picture Option Grid had more impact among women of lower SES and health literacy. Neither intervention affected concordance, treatment choice, or anxiety.
Conclusions: Paper-based conversation aids improved key outcomes over usual care. The Picture Option Grid had more impact among disadvantaged patients.
Lay summary: The objective of this study was to understand how to help women with lower incomes or less formal education to make breast cancer surgery choices. Compared with usual care, a conversation aid with pictures and text led to higher knowledge. It improved the decision process and shared decision making (SDM) and lowered decision regret. A text-only conversation aid led to an improved decision process, more coordinated care, and higher SDM compared to usual care. The conversation aid with pictures was more helpful for women with lower income or less formal education. Conversation aids with pictures and text helped women make better breast cancer surgery choices.
Trial registration: ClinicalTrials.gov NCT03136367.
Keywords: breast cancer disparities; breast cancer surgery; conversation aids; decision support techniques; lower educational attainment; lower health literacy; lower socioeconomic status; pictorial superiority.
© 2020 The Authors. Cancer published by Wiley Periodicals LLC on behalf of American Cancer Society.
Conflict of interest statement
Glyn Elwyn and Marie‐Anne Durand have developed the Option Grid patient decision aids, which are licensed to EBSCO Health; they receive consulting income from EBSCO Health and may receive royalties in the future. A. James O’Malley reports grants from the National Institutes of Health, the Agency for Healthcare Research and Quality, and the Patient‐Centered Outcomes Research Institute. Mary C. Politi reports grants from Merck outside the submitted work. Catherine H. Saunders holds a copyright in the consideRATE suite of tools. Karen Sepucha received salary support from 2014 to 2018 as a member of the scientific advisory board for Healthwise, a not‐for‐profit foundation that develops and distributes patient education and decision support materials; she also reports grants from the Agency for Healthcare Research and Quality, the Patient‐Centered Outcomes Research Institute, and the Patrick and Catherine Weldon Donaghue Medical Research Foundation outside the submitted work. Richard J. Barth reports grants and other from CairnSurgical, Inc, and grants from the National Institutes of Health outside the submitted work; in addition, Barth has a patent licensed to Dartmouth College. The other authors made no disclosures.
Figures
References
-
- Hurd TC, James T, Foster JM. Factors that affect breast cancer treatment: underserved and minority populations. Surg Oncol Clin N Am. 2005;14:119‐130, vii. - PubMed
-
- Bradley CJ, Given CW, Roberts C. Race, socioeconomic status, and breast cancer treatment and survival. J Natl Cancer Inst. 2002;94:490‐496. - PubMed
-
- Cross CK, Harris J, Recht A. Race, socioeconomic status, and breast carcinoma in the U.S: what have we learned from clinical studies. Cancer. 2002;95:1988‐1999. - PubMed
-
- Chen JY, Diamant AL, Thind A, Maly RC. Determinants of breast cancer knowledge among newly diagnosed, low‐income, medically underserved women with breast cancer. Cancer. 2008;112:1153‐1161. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
