

Prevalence and Population-Attributable Risk for Chronic Airflow Obstruction in a Large Multinational Study
- PMID: 33171069
- PMCID: PMC8456536
- DOI: 10.1164/rccm.202005-1990OC
Prevalence and Population-Attributable Risk for Chronic Airflow Obstruction in a Large Multinational Study
Abstract
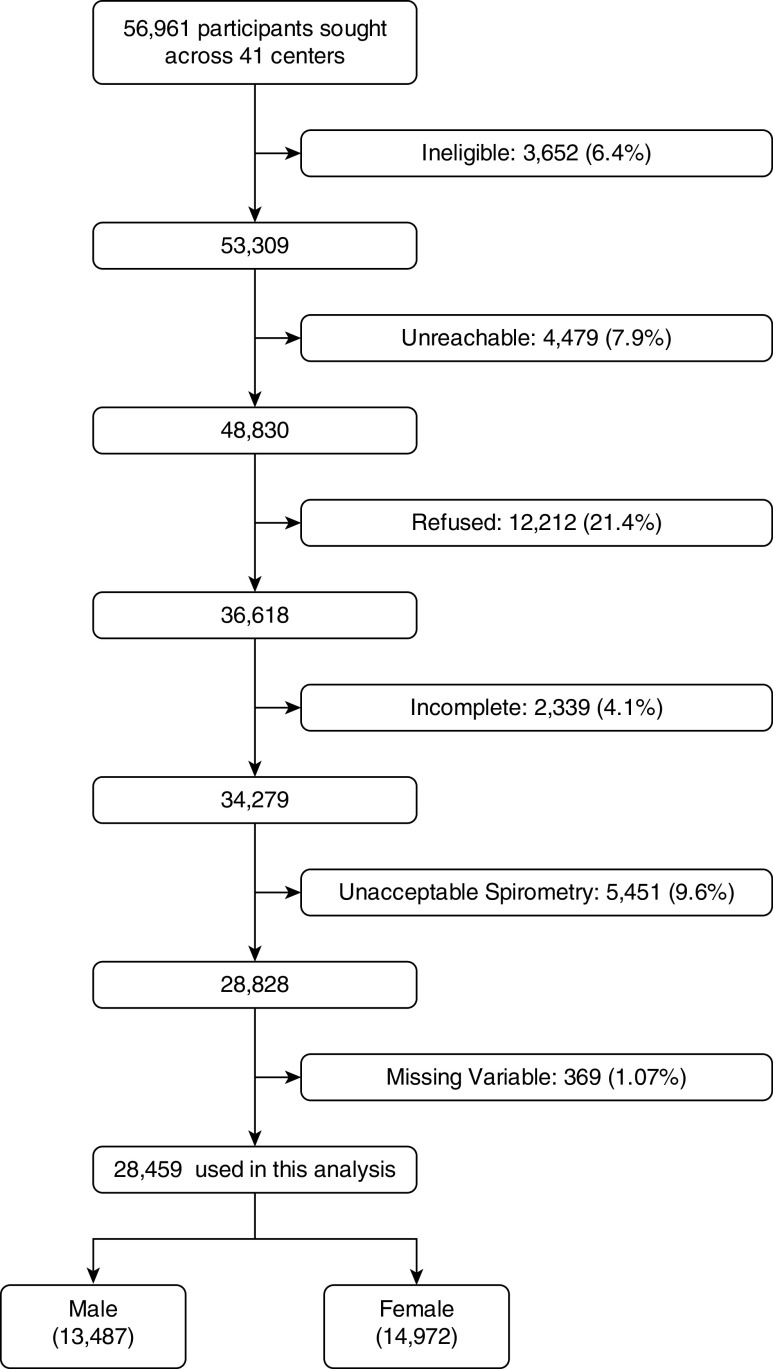
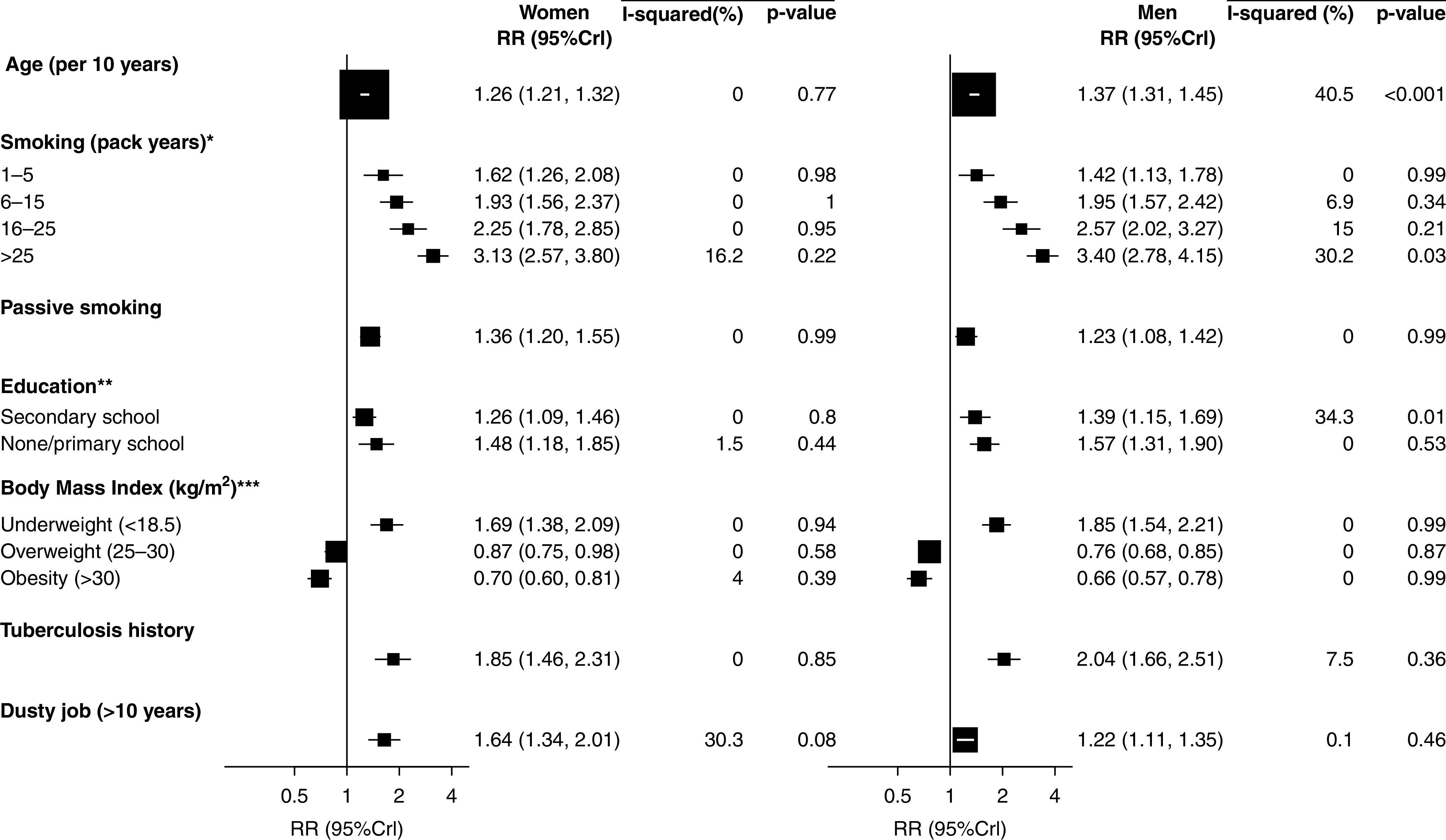
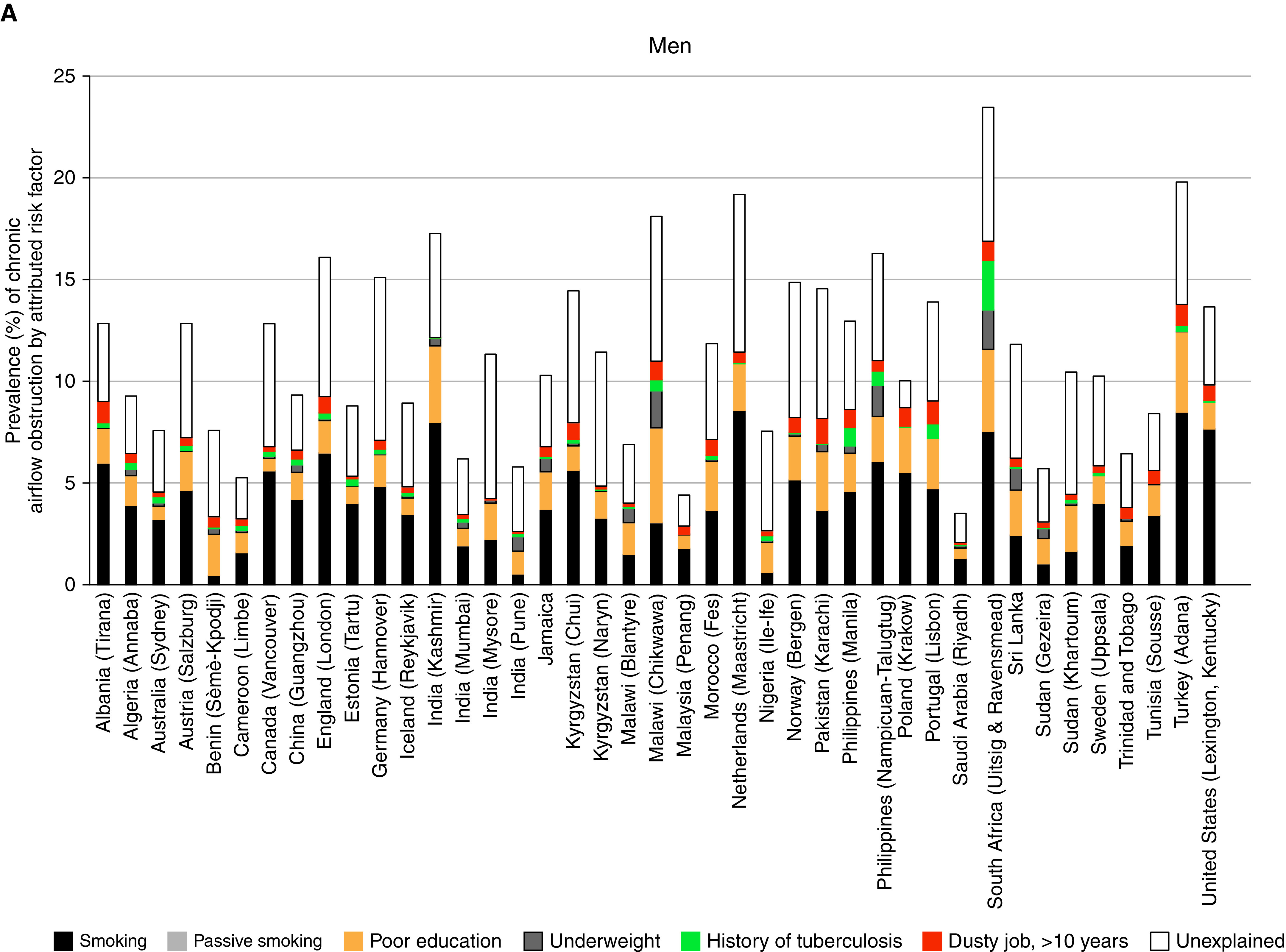
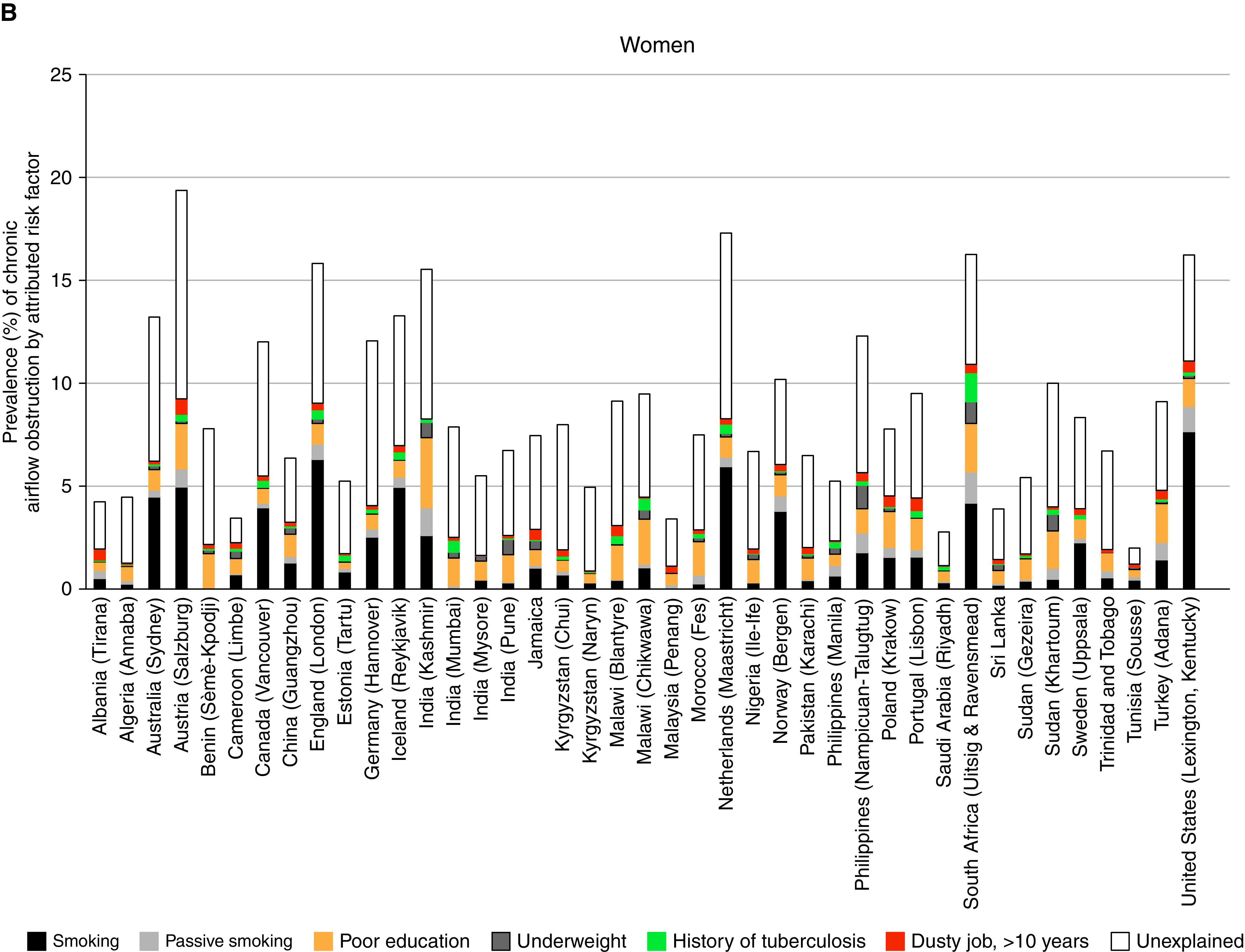
Rationale: The Global Burden of Disease program identified smoking and ambient and household air pollution as the main drivers of death and disability from chronic obstructive pulmonary disease (COPD). Objectives: To estimate the attributable risk of chronic airflow obstruction (CAO), a quantifiable characteristic of COPD, due to several risk factors. Methods: The Burden of Obstructive Lung Disease study is a cross-sectional study of adults, aged ≥40, in a globally distributed sample of 41 urban and rural sites. Based on data from 28,459 participants, we estimated the prevalence of CAO, defined as a postbronchodilator FEV1-to-FVC ratio less than the lower limit of normal, and the relative risks associated with different risk factors. Local relative risks were estimated using a Bayesian hierarchical model borrowing information from across sites. From these relative risks and the prevalence of risk factors, we estimated local population attributable risks. Measurements and Main Results: The mean prevalence of CAO was 11.2% in men and 8.6% in women. The mean population attributable risk for smoking was 5.1% in men and 2.2% in women. The next most influential risk factors were poor education levels, working in a dusty job for ≥10 years, low body mass index, and a history of tuberculosis. The risk of CAO attributable to the different risk factors varied across sites. Conclusions: Although smoking remains the most important risk factor for CAO, in some areas, poor education, low body mass index, and passive smoking are of greater importance. Dusty occupations and tuberculosis are important risk factors at some sites.
Keywords: Burden of Obstructive Lung Disease (BOLD) study; chronic airflow obstruction; multinational study; population-attributable risk.
Figures
Comment in
-
Chronic Obstructive Pulmonary Disease: Is Social Injustice the Elephant in the Room?Am J Respir Crit Care Med. 2021 Jun 1;203(11):1331-1332. doi: 10.1164/rccm.202011-4114ED. Am J Respir Crit Care Med. 2021. PMID: 33233915 Free PMC article. No abstract available.
References
-
- United Nations General Assembly. New York: United Nations: 2012. Resolution adopted by the general assembly on 19 September 2011 66/2. Political declaration of the high-level meeting of the general assembly on the prevention and control of non-communicable diseases.
-
- Murray CJL, Vos T, Lozano R, Naghavi M, Flaxman AD, Michaud C, et al. Disability-adjusted life years (DALYs) for 291 diseases and injuries in 21 regions, 1990-2010: a systematic analysis for the Global Burden of Disease Study 2010. Lancet . 2012;380:2197–2223. - PubMed
-
- Wilson D, Adams R, Appleton S, Ruffin R. Difficulties identifying and targeting COPD and population-attributable risk of smoking for COPD: a population study. Chest . 2005;128:2035–2042. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
