

Daylight Photodynamic Therapy: An Update
- PMID: 33171665
- PMCID: PMC7664668
- DOI: 10.3390/molecules25215195
Daylight Photodynamic Therapy: An Update
Abstract
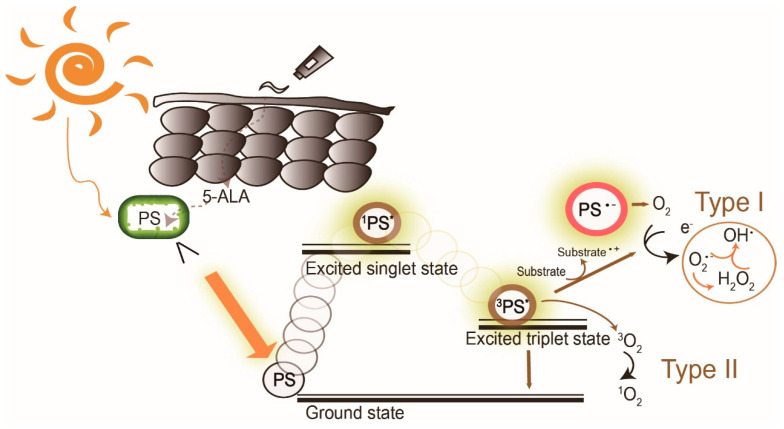
Daylight photodynamic therapy (dPDT) uses sunlight as a light source to treat superficial skin cancer. Using sunlight as a therapeutic device has been present for centuries, forming the basis of photodynamic therapy in the 20th century. Compared to conventional PDT, dPDT can be a less painful, more convenient and an effective alternative. The first clinical uses of dPDT on skin cancers began in Copenhagen in 2008. Currently, aminolevulinic acid-mediated dPDT has been approved to treat actinic keratosis patients in Europe. In this review article, we introduce the history and mechanism of dPDT and focus on the pros and cons of dPDT in treating superficial skin cancers. The future applications of dPDT on other skin diseases are expected to expand as conventional PDT evolves.
Keywords: actinic keratosis; aminolevulinic acid; daylight; history; nonmelanoma skin cancer; photodynamic therapy.
Conflict of interest statement
The authors declare no conflict of interest.
Figures

References
-
- Morton C.A., Szeimies R.M., Basset-Seguin N., Calzavara-Pinton P., Gilaberte Y., Haedersdal M., Hofbauer G.F.L., Hunger R.E., Karrer S., Piaserico S., et al. European Dermatology Forum guidelines on topical photodynamic therapy 2019 Part 1: Treatment delivery and established indications—Actinic keratoses, Bowen’s disease and basal cell carcinomas. J. Eur. Acad. Dermatol. Venereol. 2019;33:2225–2238. doi: 10.1111/jdv.16017. - DOI - PubMed
Publication types
MeSH terms
Substances
Supplementary concepts
Grants and funding
- B108-K102/National Cheng Kung University
- NCKUH-10902032/National Cheng Kung University Hospital
- MOST 109-2327-B-006-005/Ministry of Science and Technology, Taiwan
- the Center of Applied Nanomedicine, National Cheng Kung University from the Featured Areas Research Center Program within the framework of the Higher Education Sprout Project/Ministry of Education
LinkOut - more resources
Full Text Sources
Miscellaneous
