

Understanding the neuroprotective effect of tranexamic acid: an exploratory analysis of the CRASH-3 randomised trial
- PMID: 33172504
- PMCID: PMC7657351
- DOI: 10.1186/s13054-020-03243-4
Understanding the neuroprotective effect of tranexamic acid: an exploratory analysis of the CRASH-3 randomised trial
Abstract
Background: The CRASH-3 trial hypothesised that timely tranexamic acid (TXA) treatment might reduce deaths from intracranial bleeding after traumatic brain injury (TBI). To explore the mechanism of action of TXA in TBI, we examined the timing of its effect on death.
Methods: The CRASH-3 trial randomised 9202 patients within 3 h of injury with a GCS score ≤ 12 or intracranial bleeding on CT scan and no significant extracranial bleeding to receive TXA or placebo. We conducted an exploratory analysis of the effects of TXA on all-cause mortality within 24 h of injury and within 28 days, excluding patients with a GCS score of 3 or bilateral unreactive pupils, stratified by severity and country income. We pool data from the CRASH-2 and CRASH-3 trials in a one-step fixed effects individual patient data meta-analysis.
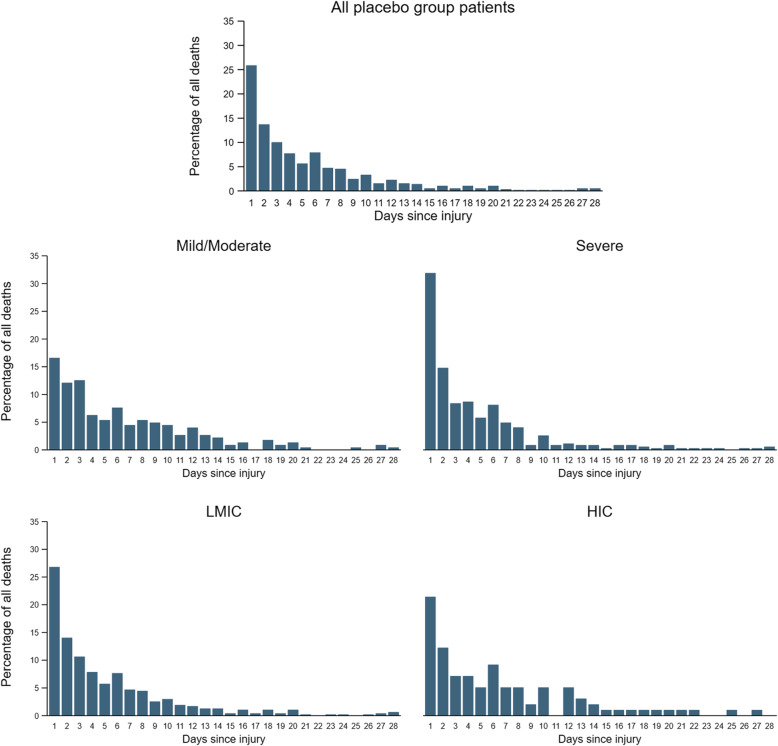
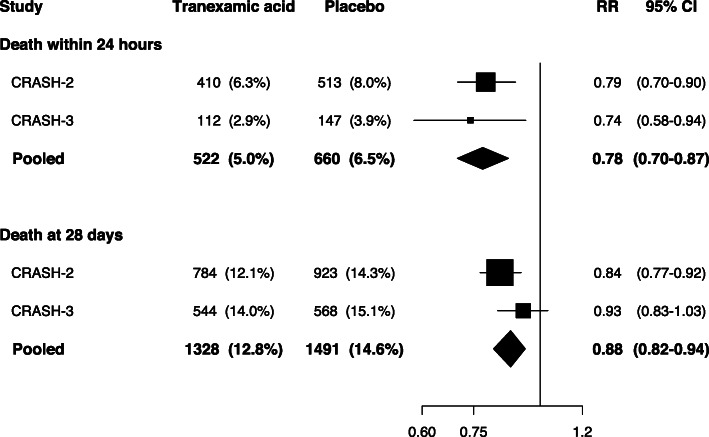
Results: There were 7637 patients for analysis after excluding patients with a GCS score of 3 or bilateral unreactive pupils. Of 1112 deaths, 23.3% were within 24 h of injury (early deaths). The risk of early death was reduced with TXA (112 (2.9%) TXA group vs 147 (3.9%) placebo group; risk ratio [RR] RR 0.74, 95% CI 0.58-0.94). There was no evidence of heterogeneity by severity (p = 0.64) or country income (p = 0.68). The risk of death beyond 24 h of injury was similar in the TXA and placebo groups (432 (11.5%) TXA group vs 421 (11.7%) placebo group; RR 0.98, 95% CI 0.69-1.12). The risk of death at 28 days was 14.0% in the TXA group versus 15.1% in the placebo group (544 vs 568 events; RR 0.93, 95% CI 0.83-1.03). When the CRASH-2 and CRASH-3 trial data were pooled, TXA reduced early death (RR 0.78, 95% CI 0.70-0.87) and death within 28 days (RR 0.88, 95% CI 0.82-0.94).
Conclusions: Tranexamic acid reduces early deaths in non-moribund TBI patients regardless of TBI severity or country income. The effect of tranexamic acid in patients with isolated TBI is similar to that in polytrauma. Treatment is safe and even severely injured patients appear to benefit when treated soon after injury.
Trial registration: ISRCTN15088122 , registered on 19 July 2011; NCT01402882 , registered on 26 July 2011.
Keywords: CRASH-3 trial; Emergence care; Epidemiology; Intracranial haemorrhage; Randomised controlled trial; Tranexamic acid; Traumatic brain injury.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- CRASH-3 Collaborators Effects of tranexamic acid on death, disability, vascular occlusive events and other morbidities in patients with acute traumatic brain injury (CRASH-3): a randomised, placebo-controlled trial. Lancet. 2019;394:1713–1723. doi: 10.1016/S0140-6736(19)32233-0. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
