

Prognostic utility of neutrophil-to-lymphocyte ratio in patients with metastatic colorectal cancer treated using different modalities
- PMID: 33173374
- PMCID: PMC7606052
- DOI: 10.3747/co.27.6573
Prognostic utility of neutrophil-to-lymphocyte ratio in patients with metastatic colorectal cancer treated using different modalities
Abstract
Introduction: Inflammation is a critical component in carcinogenesis. The neutrophil-to-lymphocyte ratio (nlr) has been retrospectively studied as a biomarker of prognosis in metastatic colorectal cancer (mcrc). Compared with a low nlr, a high nlr is associated with worse prognosis. In the present study, we compared real-world survival for patients with mcrc based on their nlr group, and we assessed the utility of the nlr in determining first-line chemotherapy and metastasectomy benefit.
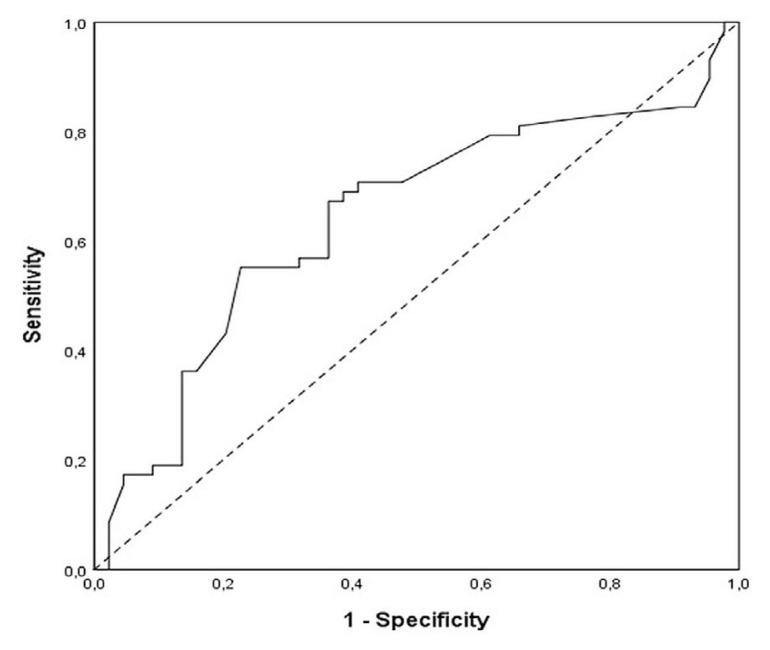
Methods: In this retrospective and descriptive analysis of patients with mcrc undergoing first-line chemotherapy in a single centre, the last systemic absolute neutrophil and lymphocyte count before treatment was used for the nlr. A receiver operating characteristic curve was used to estimate the nlr cut-off value, dividing the patients into low and high nlr groups. Median overall survival (mos) was compared using Kaplan-Meier curves and the log-rank test. A multivariate analysis was performed using a Cox regression model.
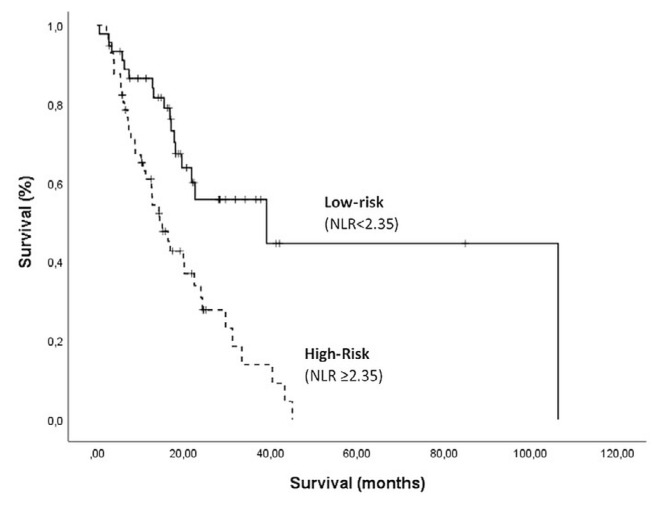
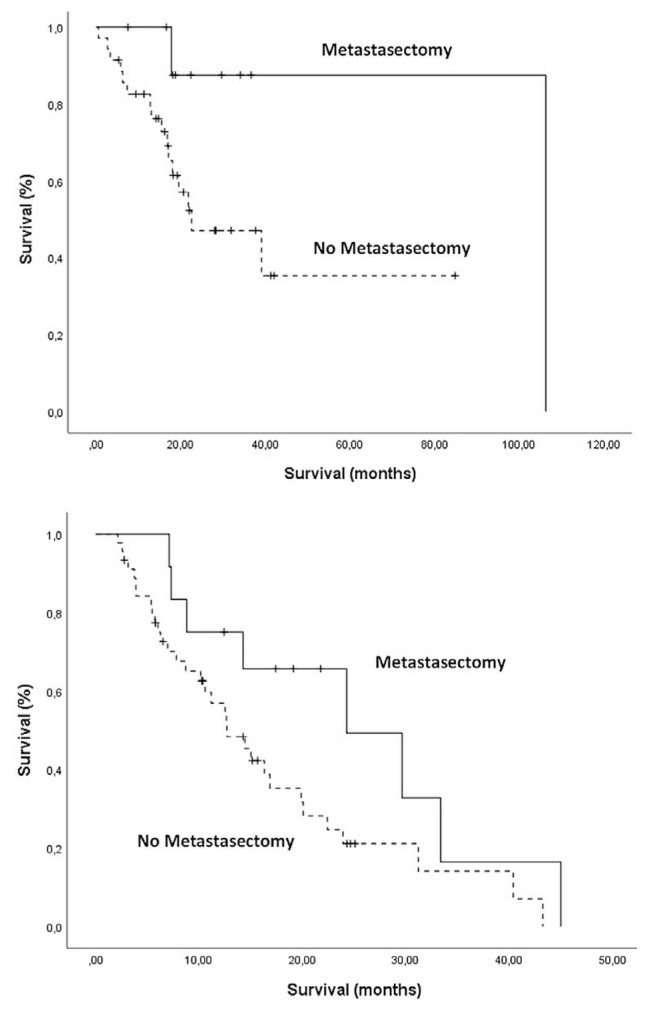
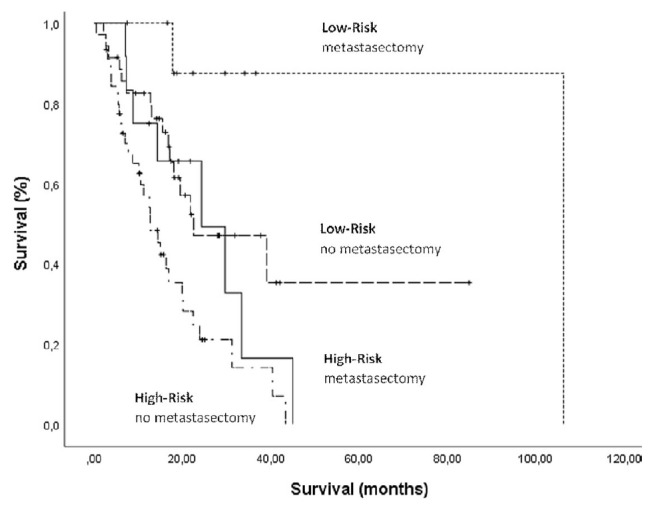
Results: The 102 analyzed patients had a median follow-up of 15 months. Regardless of systemic therapy, approximately 20% of patients underwent metastasectomy. The nlr cut-off was established at 2.35, placing 45 patients in the low-risk group (nlr < 2.35) and 57 in the high-risk group (nlr ≥ 2.35). The Kaplan-Meier analysis showed a mos of 39.1 months in the low-risk group and 14.4 months in the high-risk group (p < 0.001). Multivariate Cox regression on the nlr estimated a hazard ratio of 3.08 (p = 0.01). Survival analysis in each risk subgroup, considering the history of metastasectomy, was also performed. In the low-risk group, mos was longer for patients undergoing metastasectomy than for those not undergoing the procedure (95.2 months vs. 22.6 months, p = 0.05). In the high-risk group, mos was not statistically different for patients undergoing or not undergoing metastasectomy (24.3 months vs. 12.7 months, p = 0.08).
Conclusions: Our real-world data analysis of nlr in patients with mcrc confirmed that this biomarker is useful in predicting survival. It also suggests that nlr is an effective tool to choose first-line treatment and to predict the benefit of metastasectomy.
Keywords: Colorectal cancer; lymphocytes; metastasectomy; metastatic; neutrophils; nlr.
2020 Multimed Inc.
Conflict of interest statement
CONFLICT OF INTEREST DISCLOSURES We have read and understood Current Oncology’s policy on disclosing conflicts of interest, and we declare that we have none.
Figures
References
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
