

Adhesive small bowel obstruction - an update
- PMID: 33173587
- PMCID: PMC7642618
- DOI: 10.1002/ams2.587
Adhesive small bowel obstruction - an update
Abstract
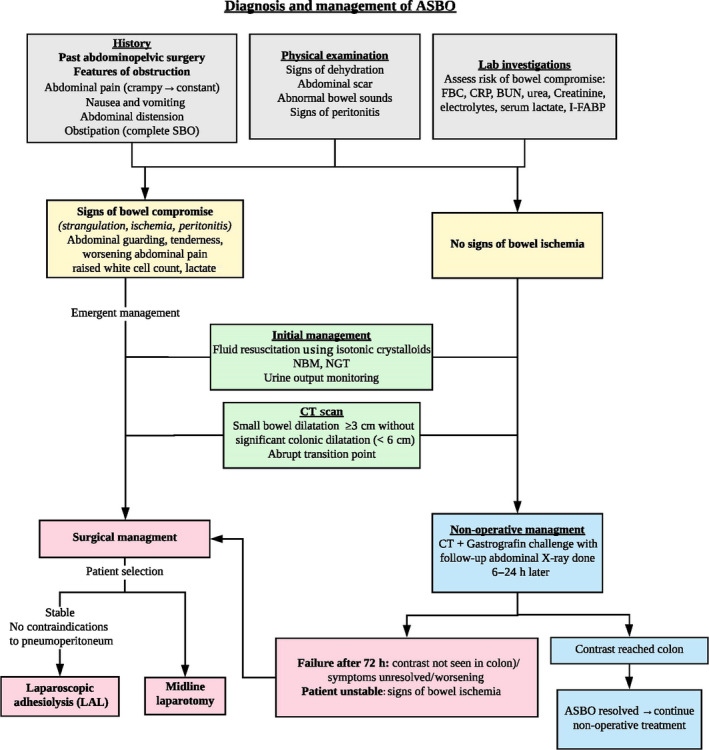
Small bowel obstruction (SBO) accounts for 12-16% of emergency surgical admissions and 20% of emergency surgical procedures. Even with the advent of laparoscopic surgery, intra-abdominal adhesions remain a significant cause of SBO, accounting for 65% of cases. History and physical examination are essential to identify signs of bowel ischemia as this indicates a need for urgent surgical exploration. Another critical aspect of evaluation includes establishing the underlying cause for obstruction and distinguishing between adhesive and non-adhesive etiologies as adhesive SBO (ASBO) can be managed non-operatively in 70-90% of patients. A patient with a history of abdominopelvic surgery along with one or more cardinal features of obstruction should be suspected to have ASBO until proven otherwise. Triad of severe pain, pain out of proportion to the clinical findings, and presence of an abdominal scar suggest possible closed-loop obstruction. Computed tomography has higher sensitivity and specificity compared to plain films and is recommended by the Bologna guidelines. Correcting fluid and electrolyte imbalance is an initial crucial step to mitigate severe hypovolemia. Patients should proceed with surgery if symptoms of bowel compromise are present, or if symptoms do not resolve or have worsened. Surgery is indicated in patients with ischemia, strangulation, perforation, peritonitis, or failure of non-operative treatment. With advances in minimal access technology and increasing experience, laparoscopic adhesiolysis is recommended. Mechanical adhesion barriers are an effective measure to prevent adhesion formation.
Keywords: Gastrointestinal tract; general surgery; intestinal obstruction; small intestine; tissue adhesion.
© 2020 The Authors. Acute Medicine & Surgery published by John Wiley & Sons Australia, Ltd on behalf of Japanese Association for Acute Medicine.
Conflict of interest statement
Approval of the research protocol: N/A. Informed consent: N/A. Registry and the registration no. of the study/trial: N/A. Animal studies: N/A. Conflict of interest: None.
Figures


References
-
- Maung AA, Johnson DC, Piper GL, et al Evaluation and management of small‐bowel obstruction: An Eastern Association for the Surgery of Trauma practice management guideline. J. Trauma Acute Care Surg. 2012; 73: S362–S369. - PubMed
-
- Millet I, Ruyer A, Alili C, et al Adhesive small‐bowel obstruction: Value of CT in identifying findings associated with the effectiveness of nonsurgical treatment. Radiology 2014; 273: 425–32. - PubMed
-
- Rami Reddy SR, Cappell MS. A systematic review of the clinical presentation, diagnosis, and treatment of small bowel obstruction. Curr. Gastroenterol. Rep. 2017; 19: 1–14. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Medical
