

High prevalence of SARS-CoV-2 antibodies in care homes affected by COVID-19: Prospective cohort study, England
- PMID: 33173854
- PMCID: PMC7644437
- DOI: 10.1016/j.eclinm.2020.100597
High prevalence of SARS-CoV-2 antibodies in care homes affected by COVID-19: Prospective cohort study, England
Abstract
Background: We investigated six London care homes experiencing a COVID-19 outbreak and found high rates of SARS-CoV-2 infection among residents and staff. Here we report follow-up investigations including antibody testing in the same care homes five weeks later.
Methods: Residents and staff in the initial investigation had a repeat nasal swab for SARS-CoV-2 RT-PCR and a blood test for SARS CoV-2 antibodies using ELISA based on SARS-CoV-2 native viral antigens derived from infected cells and virus neutralisation.
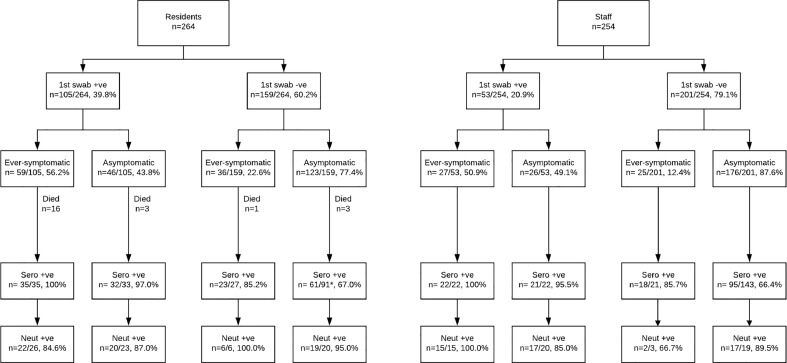
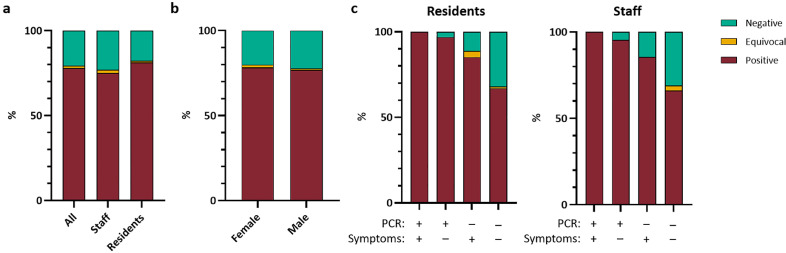
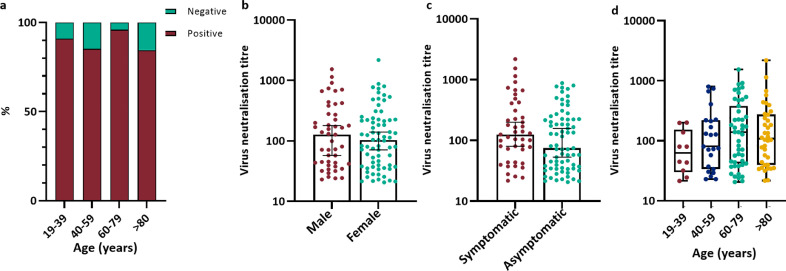
Findings: Of the 518 residents and staff in the initial investigation, 186/241 (77.2%) surviving residents and 208/254 (81.9%) staff underwent serological testing. Almost all SARS-CoV-2 RT-PCR positive residents and staff were seropositive five weeks later, whether symptomatic (residents 35/35, 100%; staff, 22/22, 100%) or asymptomatic (residents 32/33, 97.0%; staff 21/22, 95.5%). Symptomatic but SARS-CoV-2 RT-PCR negative residents and staff also had high seropositivity rates (residents 23/27, 85.2%; staff 18/21, 85.7%), as did asymptomatic RT-PCR negative individuals (residents 61/91, 67.0%; staff 95/143, 66.4%). Neutralising antibody was detected in 118/132 (89.4%) seropositive individuals and was not associated with age or symptoms. Ten residents (10/79 re-tested, 12.7%) remained RT-PCR positive but with higher RT-PCR cycle threshold values; 7/10 had serological testing and all were seropositive. New infections were detected in three residents and one staff.
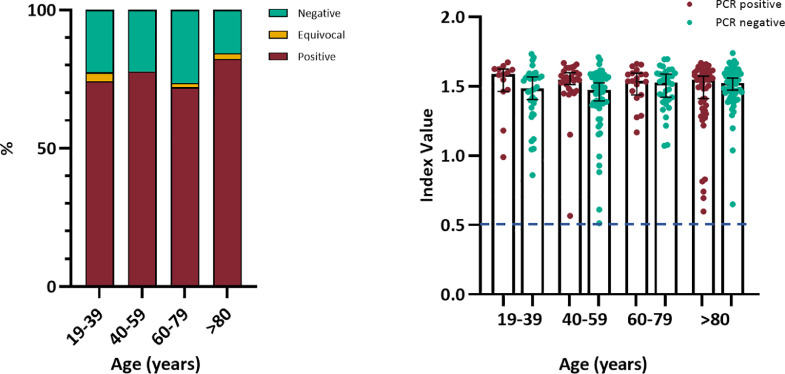
Interpretation: RT-PCR provides a point prevalence of SARS-CoV-2 infection but significantly underestimates total exposure in outbreak settings. In care homes experiencing large COVID-19 outbreaks, most residents and staff had neutralising SARS-CoV-2 antibodies, which was not associated with age or symptoms.
Funding: PHE.
Crown Copyright © 2020 Published by Elsevier Ltd.
Conflict of interest statement
The authors have nothing to declare.
Figures
Similar articles
-
Reinfection with new variants of SARS-CoV-2 after natural infection: a prospective observational cohort in 13 care homes in England.Lancet Healthy Longev. 2021 Dec;2(12):e811-e819. doi: 10.1016/S2666-7568(21)00253-1. Epub 2021 Dec 1. Lancet Healthy Longev. 2021. PMID: 34873592 Free PMC article.
-
Investigation of SARS-CoV-2 outbreaks in six care homes in London, April 2020.EClinicalMedicine. 2020 Sep;26:100533. doi: 10.1016/j.eclinm.2020.100533. Epub 2020 Sep 9. EClinicalMedicine. 2020. PMID: 32923993 Free PMC article.
-
Infection and transmission of SARS-CoV-2 in London care homes reporting no cases or outbreaks of COVID-19: Prospective observational cohort study, England 2020.Lancet Reg Health Eur. 2021 Apr;3:100038. doi: 10.1016/j.lanepe.2021.100038. Epub 2021 Jan 22. Lancet Reg Health Eur. 2021. PMID: 33870248 Free PMC article.
-
SARS-CoV-2 seropositivity and subsequent infection risk in healthy young adults: a prospective cohort study.Lancet Respir Med. 2021 Jul;9(7):712-720. doi: 10.1016/S2213-2600(21)00158-2. Epub 2021 Apr 15. Lancet Respir Med. 2021. PMID: 33865504 Free PMC article.
-
Mass testing after a single suspected or confirmed case of COVID-19 in London care homes, April-May 2020: implications for policy and practice.Age Ageing. 2021 May 5;50(3):649-656. doi: 10.1093/ageing/afab054. Age Ageing. 2021. PMID: 33620453 Free PMC article.
Cited by
-
Persistence of Neutralizing Antibodies and Clinical Protection up to 12 Months After Severe Acute Respiratory Syndrome Coronavirus 2 Infection in the Elderly.Open Forum Infect Dis. 2022 Nov 11;9(11):ofac613. doi: 10.1093/ofid/ofac613. eCollection 2022 Nov. Open Forum Infect Dis. 2022. PMID: 36467299 Free PMC article.
-
Occurrence and transmission potential of asymptomatic and presymptomatic SARS-CoV-2 infections: Update of a living systematic review and meta-analysis.PLoS Med. 2022 May 26;19(5):e1003987. doi: 10.1371/journal.pmed.1003987. eCollection 2022 May. PLoS Med. 2022. PMID: 35617363 Free PMC article.
-
Attribution of nosocomial seeding to long-term care facility COVID-19 outbreaks.Epidemiol Infect. 2023 Oct 25;151:e191. doi: 10.1017/S0950268823001565. Epidemiol Infect. 2023. PMID: 37876042 Free PMC article.
-
Antibodies to SARS-CoV-2 protect against re-infection during outbreaks in care homes, September and October 2020.Euro Surveill. 2021 Feb;26(5):2100092. doi: 10.2807/1560-7917.ES.2021.26.5.2100092. Euro Surveill. 2021. PMID: 33541486 Free PMC article.
-
Disparities of SARS-CoV-2 Nucleoprotein-Specific IgG in Healthcare Workers in East London, UK.Front Med (Lausanne). 2021 Apr 27;8:642723. doi: 10.3389/fmed.2021.642723. eCollection 2021. Front Med (Lausanne). 2021. PMID: 33987193 Free PMC article.
References
-
- Office for National Statistics (ONS). Deaths involving COVID-19 in the care sector, England and Wales: deaths occurring up to 12 June 2020 and registered up to 20 June 2020 (provisional). 03 July 2020. (Accessed 04 September 2020, 2020. Available at: https://www.ons.gov.uk/peoplepopulationandcommunity/birthsdeathsandmarri.... Accessed: 05 September 2020.
-
- Public Health England. National COVID-19 surveillance reports 2020. Available at: https://www.gov.uk/government/publications/national-covid-19-surveillanc.... Accessed: 05 September 2020.
-
- Lerner A.M., Eisinger R.W., Lowy D.R. The COVID-19 serology studies workshop: recommendations and challenges. Immunity. 2020 https://www.cell.com/immunity/pdf/S1074-7613(20)30267-3.pdf Available at: Accessed: 05 September 2020. - PMC - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
