

This is a preprint.
Racial and Ethnic Disparities in Access to Health Care Among Adults in the United States: A 20-Year National Health Interview Survey Analysis, 1999-2018
- PMID: 33173905
- PMCID: PMC7654899
- DOI: 10.1101/2020.10.30.20223420
Racial and Ethnic Disparities in Access to Health Care Among Adults in the United States: A 20-Year National Health Interview Survey Analysis, 1999-2018
Update in
-
Trends in Differences in Health Status and Health Care Access and Affordability by Race and Ethnicity in the United States, 1999-2018.JAMA. 2021 Aug 17;326(7):637-648. doi: 10.1001/jama.2021.9907. JAMA. 2021. PMID: 34402830 Free PMC article.
Abstract
Importance: Racial and ethnic disparities plague the US health care system despite efforts to eliminate them. To understand what has been achieved amid these efforts, a comprehensive study from the population perspective is needed.
Objectives: To determine trends in rates and racial/ethnic disparities of key access to care measures among adults in the US in the last two decades.
Design: Cross-sectional.
Setting: Data from the National Health Interview Survey, 1999-2018.
Participants: Individuals >18 years old.
Exposure: Race and ethnicity: non-Hispanic Black, non-Hispanic Asian, non-Hispanic White, Hispanic.
Main outcome and measures: Rates of lack of insurance coverage, lack of a usual source of care, and foregone/delayed medical care due to cost. We also estimated the gap between non-Hispanic White and the other subgroups for these outcomes.
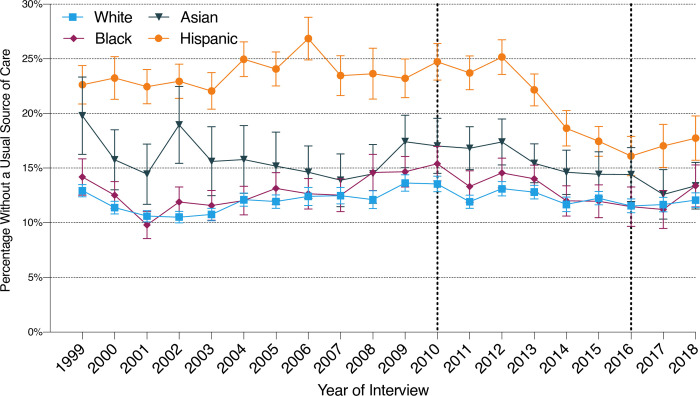
Results: We included 596,355 adults, of which 69.7% identified as White, 11.8% as Black, 4.7% as Asian, and 13.8% as Hispanic. The proportion uninsured and the rates of lacking a usual source of care remained stable across all 4 race/ethnicity subgroups up to 2009, while rates of foregone/delayed medical care due to cost increased. Between 2010 and 2015, the percentage of uninsured diminished for all, with the steepest reduction among Hispanics (-2.1% per year). In the same period, rates of no usual source of care declined only among Hispanics (-1.2% per year) while rates of foregone/delayed medical care due to cost decreased for all. No substantial changes were observed from 2016-2018 in any outcome across subgroups. Compared with 1999, in 2018 the rates of foregone/delayed medical care due to cost were higher for all (+3.1% among Whites, +3.1% among Blacks, +0.5% among Asians, and +2.2% among Hispanics) without significant change in gaps; rates of no usual source of care were not significantly different among Whites or Blacks but were lower among Hispanics (-4.9%) and Asians (-6.4%).
Conclusions and relevance: Insurance coverage increased for all, but millions of individuals remained uninsured or underinsured with increasing rates of unmet medical needs due to cost. Those identifying as non-Hispanic Black and Hispanic continue to experience more barriers to health care services compared with non-Hispanic White individuals.
Key points: Question: In the last 2 decades, what has been achieved in reducing barriers to access to care and race/ethnicity-associated disparities?Findings: Using National Health Interview Survey data from 1999-2018, we found that insurance coverage increased across all 4 major race/ethnicity groups. However, rates of unmet medical needs due to cost increased without reducing the respective racial/ethnic disparities, and little-to-no change occurred in rates of individuals who have no usual source of care.Meaning: Despite increased coverage, millions of Americans continued to experience barriers to access to care, which were disproportionately more prevalent among those identifying as Black or Hispanic.
Figures


References
-
- Chou CH, Tulolo A, Raver EW, Hsu CH, Young G. Effect of race and health insurance on health disparities: results from the National Health Interview Survey 2010. J Health Care Poor Underserved. 2013;24(3):1353–1363. - PubMed
-
- Monheit AC, Vistnes JP. Race/ethnicity and health insurance status: 1987 and 1996. Med Care Res Rev. 2000;57 Suppl 1:11–35. - PubMed
-
- 2018 National Healthcare Quality and Disparities Report. Rockville, MD: U.S. Department of Health and Human Services; 2019.
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous