

Prescription Opioid Use and Risk for Major Depressive Disorder and Anxiety and Stress-Related Disorders: A Multivariable Mendelian Randomization Analysis
- PMID: 33175090
- PMCID: PMC7658804
- DOI: 10.1001/jamapsychiatry.2020.3554
Prescription Opioid Use and Risk for Major Depressive Disorder and Anxiety and Stress-Related Disorders: A Multivariable Mendelian Randomization Analysis
Abstract
Importance: Growing evidence suggests that prescription opioid use affects depression and anxiety disorders; however, observational studies are subject to confounding, making causal inference and determining the direction of these associations difficult.
Objective: To investigate the potential bidirectional associations between the genetic liability for prescription opioid and other nonopioid pain medications and both major depressive disorder (MDD) and anxiety and stress-related disorders (ASRD) using genetically based methods.
Design, setting, and participants: We performed 2-sample mendelian randomization (MR) using summary statistics from genome-wide association studies (GWAS) to assess potential associations of self-reported prescription opioid and nonopioid analgesics, including nonsteroidal anti-inflammatories (NSAIDs) and acetaminophen-like derivatives use with MDD and ASRD. The GWAS data were derived from participants of predominantly European ancestry included in observational cohorts. Data were analyzed February 20, 2020, to May 4, 2020.
Main outcomes and measures: Major depressive disorder, ASRD, and self-reported pain medications (opioids, NSAIDs, anilides, and salicylic acid).
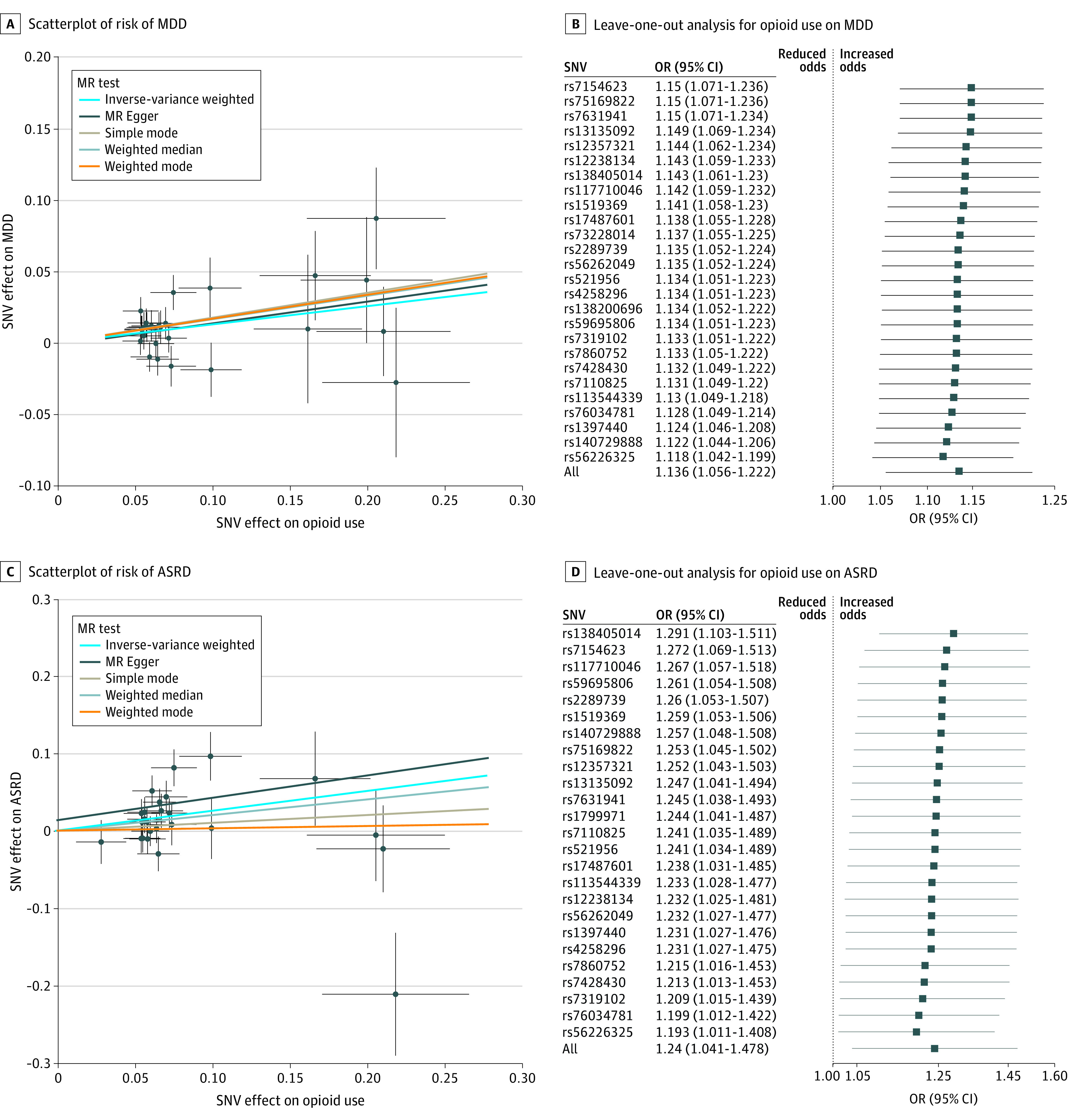
Results: The GWAS data were derived from participants of predominantly European ancestry included in the population-based UK Biobank and Lundbeck Foundation Initiative for Integrative Psychiatric Research studies: approximately 54% of the initial UK Biobank sample and 55.6% of the Lundbeck Foundation Initiative for Integrative Psychiatric Research sample selected for the ASRD GWAS were women. In a combined sample size of 737 473 study participants, single-variable MR showed that genetic liability for increased prescription opioid use was associated with increased risk of both MDD (odds ratio [OR] per unit increase in log odds opioid use, 1.14; 95% CI, 1.06-1.22; P < .001) and ASRD (OR, 1.24; 95% CI, 1.07-1.44; P = .004). Using multivariable MR, these opioid use estimates remained after accounting for other nonopioid pain medications (MDD OR, 1.14; 95% CI, 1.04-1.25; P = .005; ASRD OR, 1.30; 95% CI, 1.08-1.46; P = .006), and in separate models, accounting for comorbid pain conditions. Bidirectional analyses showed that genetic liability for MDD but not ASRD was associated with increased prescription opioid use risk (OR, 1.18; 95% CI, 1.08-1.30; P < .001). These estimates were generally consistent across single-variable and multivariable inverse variance-weighted (MV-IVW) and MR-Egger sensitivity analyses. Pleiotropy-robust methods did not indicate bias in any MV-IVW estimates.
Conclusions and relevance: The findings of this mendelian randomization analysis suggest evidence for potential causal associations between the genetic liability for increased prescription opioid use and the risk for MDD and ASRD. While replication studies are necessary, these findings may inform prevention and intervention strategies directed toward the opioid epidemic and depression.
Conflict of interest statement
Figures

References
-
- US Centers for Disease Control and Prevention Understanding the epidemic: drug overdose deaths in the United States continue to increase in 2015. Published 2011. Updated December 19, 2018. Accessed November 5, 2019. https://www.cdc.gov/drugoverdose/epidemic/
-
- Scholl L SP, Kariisa M, Wilson N, Baldwin G.. Drug and Opioid-Involved Overdose Deaths: United States, 2013–2017. MMWR Morb Mortal Wkly Rep website. Published; 2019. Accessed July 15, 2020. https://www.cdc.gov/mmwr/volumes/67/wr/mm675152e1.htm
-
- NIDA Opioid overdose crisis. Published 2019. Accessed November 6, 2019. https://www.drugabuse.gov/drugs-abuse/opioids/opioid-overdose-crisis.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
