

Patient-reported causes of distress predict disparities in time to evaluation and time to treatment after breast cancer diagnosis
- PMID: 33175437
- PMCID: PMC7897266
- DOI: 10.1002/cncr.33310
Patient-reported causes of distress predict disparities in time to evaluation and time to treatment after breast cancer diagnosis
Abstract
Background: We examined whether the National Comprehensive Cancer Network distress thermometer (DT), a patient-reported outcome measure, could be used to identify levels and causes of distress associated with racial/ethnic disparities in time to care among patients with breast cancer.
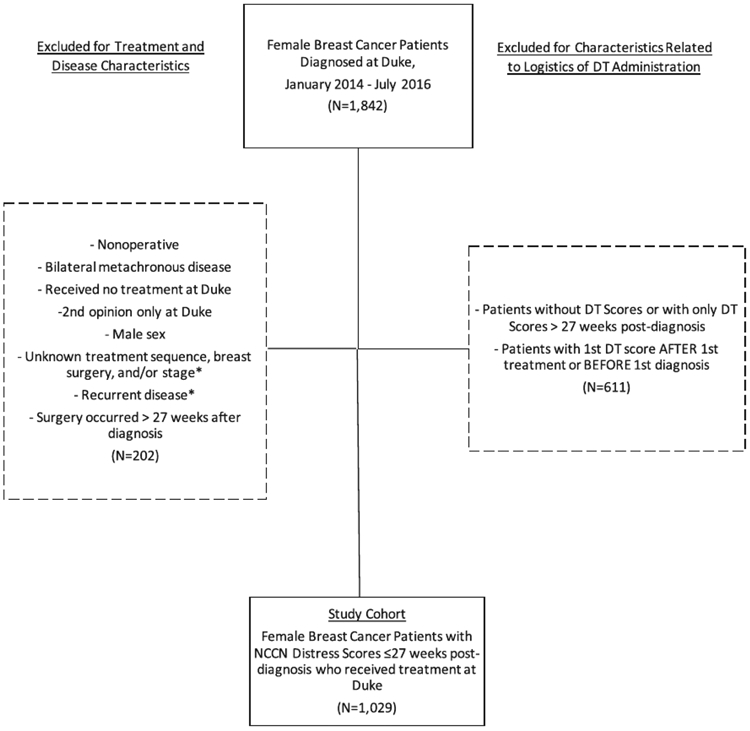
Methods: We identified women aged ≥18 years with stage 0-IV breast cancer who were diagnosed in a single health system between January 2014 and July 2016. The baseline visit was defined as the first postdiagnosis, pretreatment clinical evaluation. Zero-inflated negative binomial (ZINB) regression (modeling non-zero DT scores and DT scores = 0) and logistic regression (modeling DT score ≥ 4, threshold for social services referral) were used to examine associations between baseline score (0 = none to 10 = extreme) and types of stressors (emotional, familial, practical, physical, spiritual) after adjustment for race/ethnicity and other characteristics. Linear regression with log transformation was used to identify predictors of time to evaluation and time to treatment.
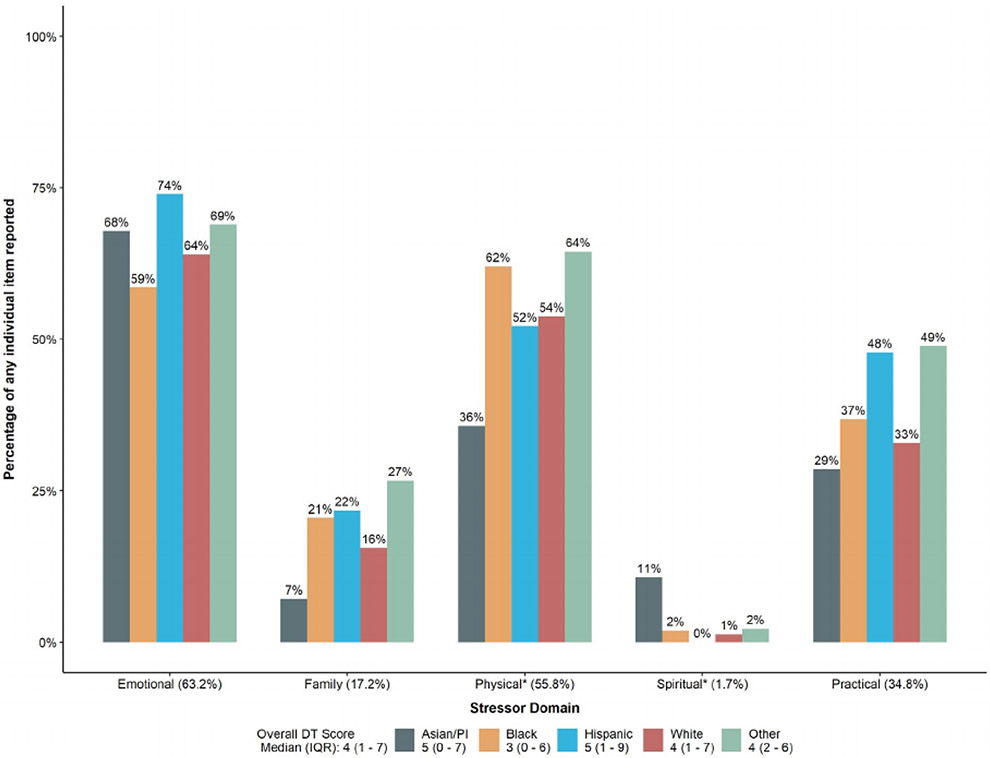
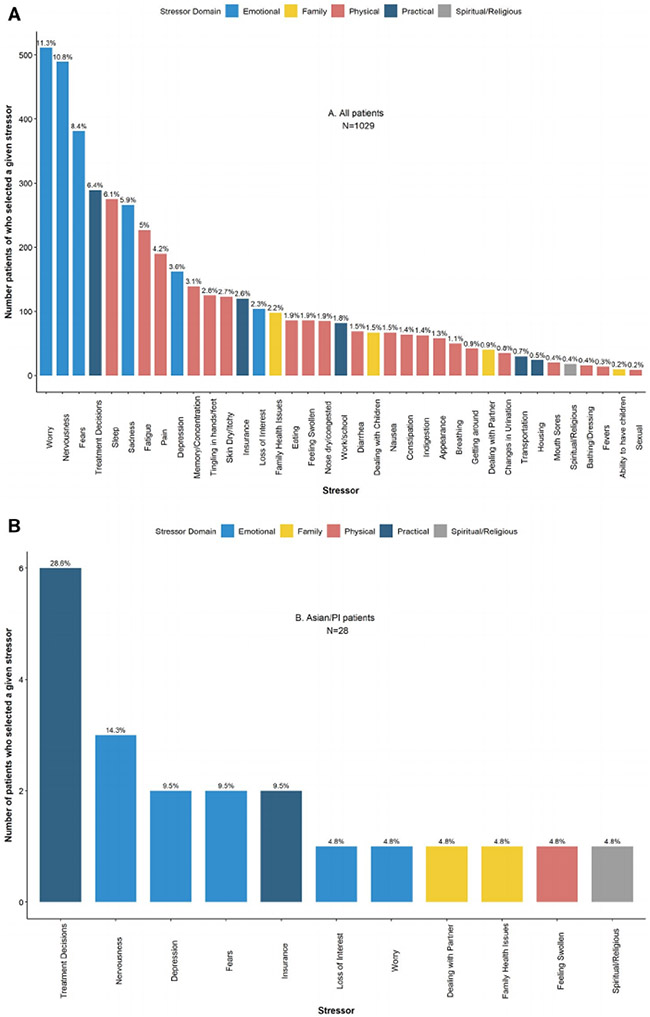
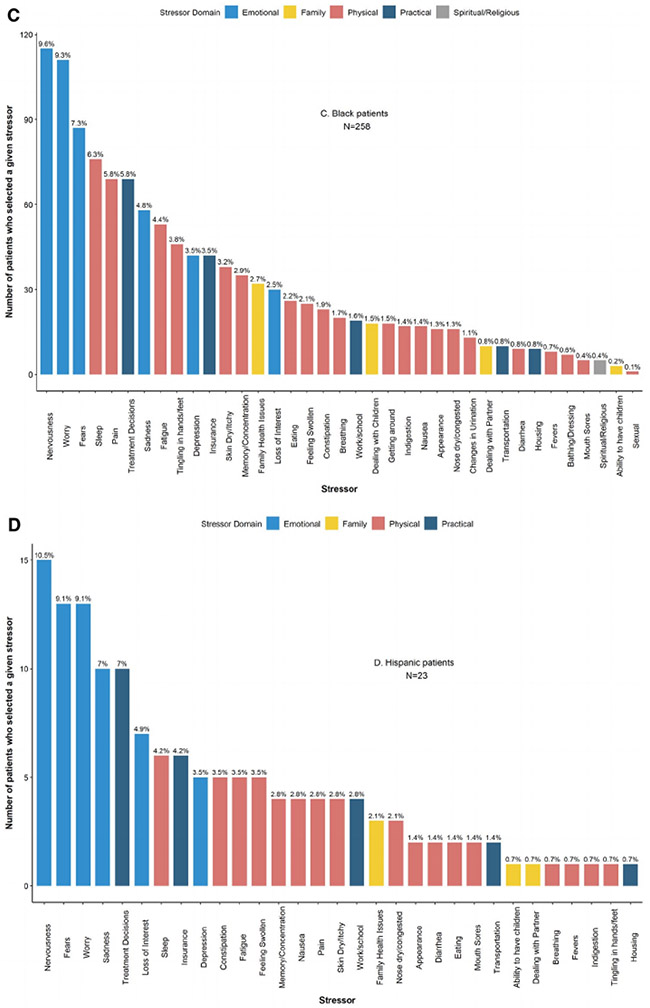
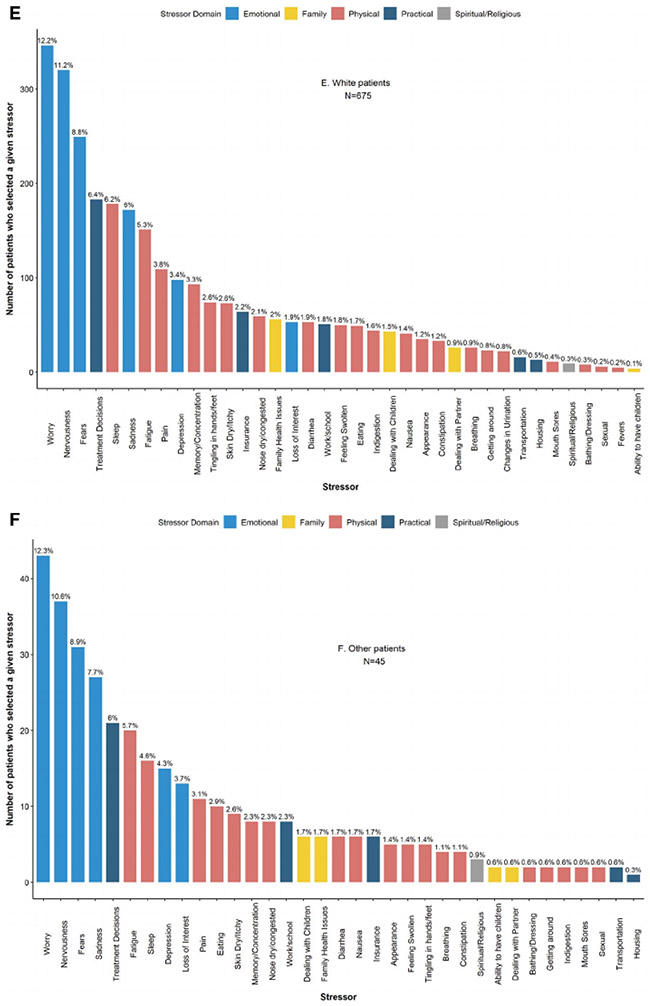
Results: A total of 1029 women were included (median baseline DT score = 4). Emotional, physical, and practical stressors were associated with distress in both the ZINB and logistic models (all P < .05). Black patients (n = 258) were more likely to report no distress than Whites (n = 675; ZINB zero model odds ratio, 2.72; 95% CI, 1.68-4.40; P < .001) despite reporting a similar number of stressors (P = .07). Higher DT scores were associated with shorter time to evaluation and time to treatment while being Black and having physical or practical stressors were associated with delays in both (all P < .05).
Conclusions: Patient-reported stressors predicted delays in time to care, but patient-reported levels of distress did not, with Black patients having delayed time to care despite reporting low levels of distress. We describe anticipatory, culturally responsive strategies for using patient-reported outcomes to address observed disparities.
Keywords: breast cancer; distress; health disparities; modifiable risk factors; patient-reported outcomes; race/ethnicity.
© 2020 American Cancer Society.
Conflict of interest statement
CONFLICT OF INTEREST DISCLOSURES
The authors made no disclosures.
Figures
References
-
- National Comprehensive Cancer Network. NCCN clinical practice guidelines in oncology: distress management, version 2.2019. Accessed 20 May 2019 http://www.nccn.org/professionals/physician_gls/pdf/distress.pdf - PMC - PubMed
-
- Gessler S, Low J, Daniells E, et al. Screening for distress in cancer patients: is the distress thermometer a valid measure in the UK and does it measure change over time? A prospective validation study. Psycho-Oncology. 2008;17:538–547. - PubMed
-
- Jacobsen PB, Donovan KA, Trask PC, et al. Screening for psychologic distress in ambulatory cancer patients. Cancer. 2005; 103: 1494–1502. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
