

Effect of Empagliflozin on Cardiovascular and Renal Outcomes in Patients With Heart Failure by Baseline Diabetes Status: Results From the EMPEROR-Reduced Trial
- PMID: 33175585
- PMCID: PMC7834911
- DOI: 10.1161/CIRCULATIONAHA.120.051824
Effect of Empagliflozin on Cardiovascular and Renal Outcomes in Patients With Heart Failure by Baseline Diabetes Status: Results From the EMPEROR-Reduced Trial
Abstract
Background: Sodium-glucose cotransporter 2 inhibitors improve outcomes in patients with heart failure with reduced ejection fraction, but additional information is needed about whether glycemic status influences the magnitude of their benefits on heart failure and renal events.
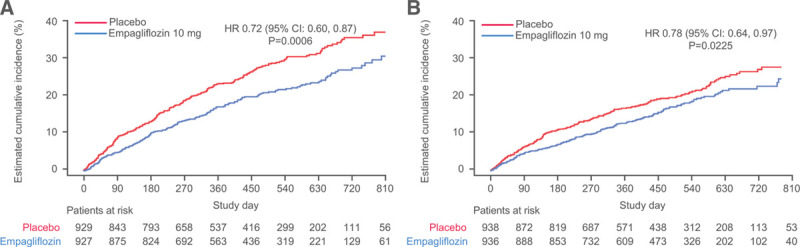
Methods: Patients with Class II-IV heart failure and a left ventricular ejection fraction ≤40% were randomized to receive empagliflozin (10 mg daily) or placebo in addition to recommended therapy. We prespecified a comparison of the effect of empagliflozin in patients with and without diabetes.
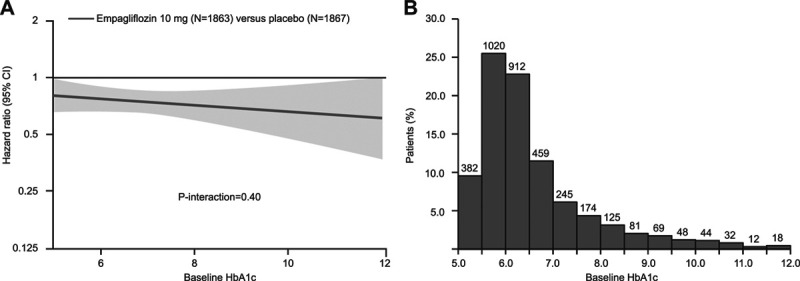
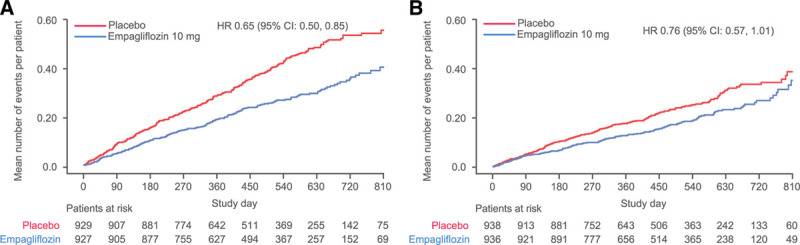
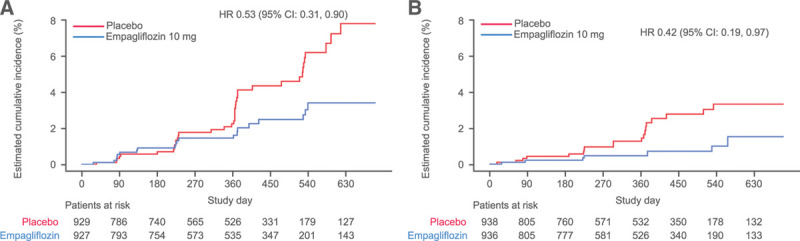
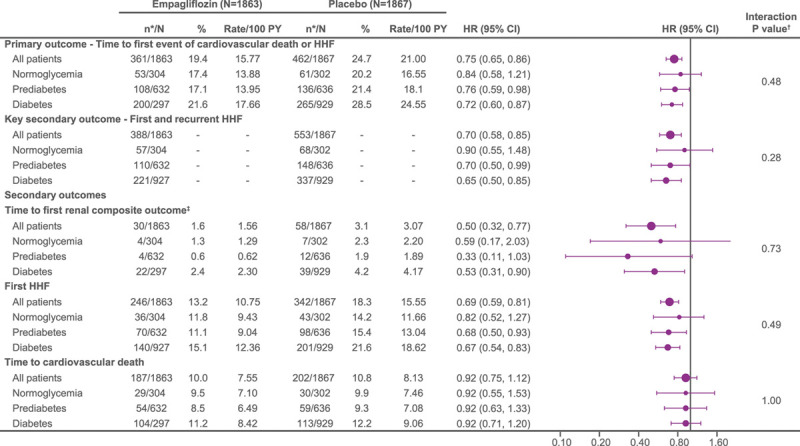
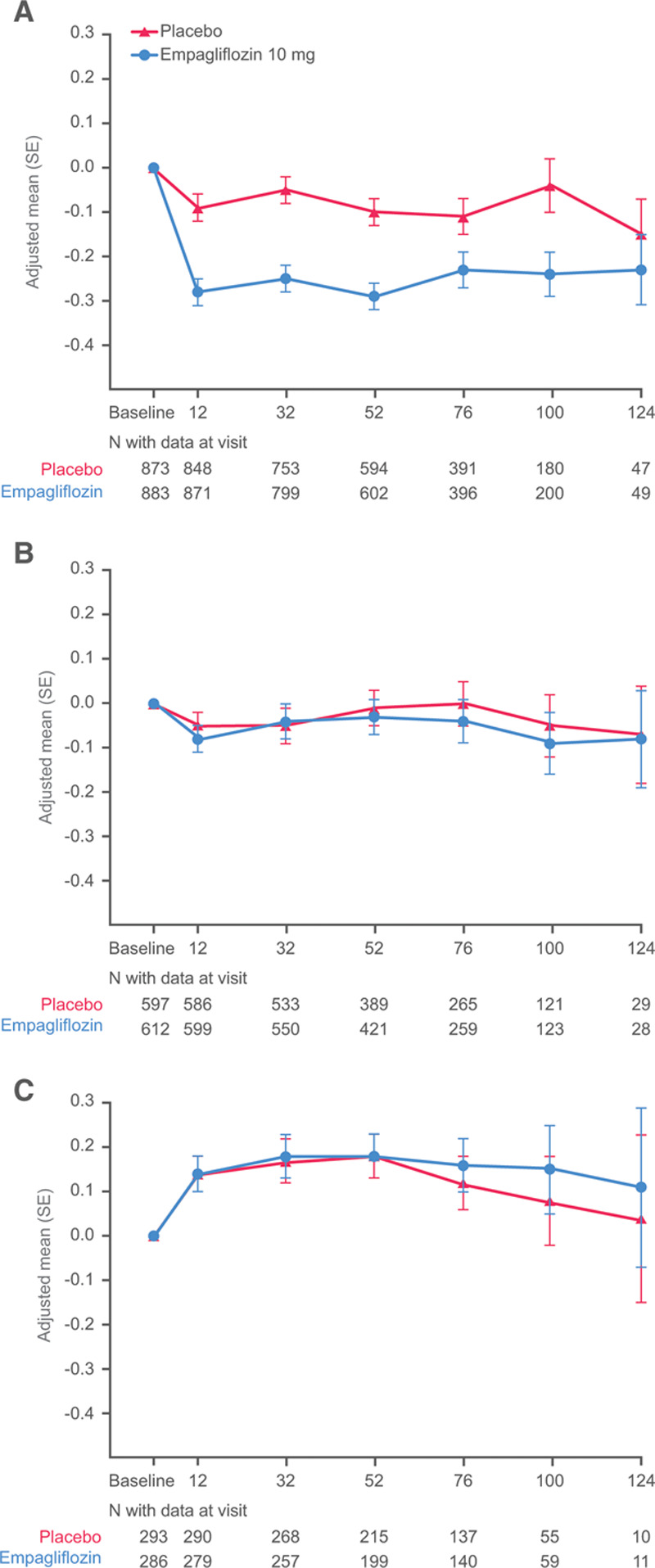
Results: Of the 3730 patients enrolled, 1856 (50%) had diabetes, 1268 (34%) had prediabetes (hemoglobin A1c [HbA1c] 5.7-6.4%), and 606 (16%) had normoglycemia (HbA1c <5.7%). The risks of the primary outcome (cardiovascular death or hospitalization for heart failure), total hospitalizations for heart failure, and adverse renal outcomes were higher in patients with diabetes, but were similar between patients with prediabetes and normoglycemia. Empagliflozin reduced the risk of the primary outcome in patients with and without diabetes (hazard ratio, 0.72 [95% CI, 0.60-0.87] and 0.78 [95% CI, 0.64-0.97], respectively, P-interaction=0.57). Patients with and without diabetes also did not differ with respect to the effect of empagliflozin on total hospitalizations for heart failure, on the decline in estimated glomerular filtration rate over time, and on the risk of serious adverse renal outcomes. Among these end points, the effects of the drug did not differ in patients with prediabetes or normoglycemia. When analyzed as a continuous variable, baseline HbA1c did not significantly modify the benefits of empagliflozin on the primary outcome (P-interaction=0.40). Empagliflozin did not lower HbA1c in patients with prediabetes or normoglycemia and was not associated with increased risk of hypoglycemia.
Conclusions: In EMPEROR-Reduced (Empagliflozin Outcome Trial in Patients With Chronic Heart Failure With Reduced Ejection Fraction), empagliflozin significantly improved cardiovascular and renal outcomes in patients with heart failure and a reduced ejection fraction, independent of baseline diabetes status and across the continuum of HbA1c. Registration: URL: https://www.clinicaltrials.gov; Unique identifier: NCT03057977.
Keywords: diabetes mellitus; empagliflozin; heart failure.
Conflict of interest statement
Dr Anker reports grants and personal fees from Vifor International and Abbott Vascular and personal fees from Astra-Zeneca, Bayer, Brahms, Boehringer Ingelheim, Cardiac Dimensions, Novartis, Occlutech, Servier, and Vifor International. Dr Butler reports consulting fees from BI, Cardior, CVRx, Foundry, G3 Pharma, Imbria, Impulse Dynamics, Innolife, Janssen, LivaNova, Luitpold, Medtronic, Merck, Novartis, NovoNordisk, Relypsa, Roche, Sanofi, Sequana Medical, V-Wave Ltd, and Vifor. Dr Filippatos reports committee member contributions in trials sponsored by Medtronic, Vifor, Servier, Novartis, and Boehringer Ingelheim. Dr Khan reports no relevant disclosures. Dr Marx is funded by the German Research Foundation SFB TRR 219 (projects M-03 and M-05); reports giving lectures for and receiving honoraria from Amgen, Boehringer Ingelheim, Sanofi-Aventis, Merck Sharp & Dohme, Bristol-Myers Squibb, AstraZeneca, Lilly, and Novo Nordisk; receiving unrestricted research grants from Boehringer Ingelheim; serving as an advisor for Amgen, Bayer, Boehringer Ingelheim, Sanofi-Aventis, Merck Sharp & Dohme, Bristol-Myers Squibb, AstraZeneca, and Novo Nordisk; serving in trial leadership for Boehringer Ingelheim and Novo Nordisk; and declining all personal compensation from pharmaceutical and device companies. Dr Lam reports research grants from Bayer, Boston Scientific, Roche Diagnostic, Medtronic, Vifor Pharma, and AstraZeneca; consulting fees from Merck, Bayer, Boston Scientific, Roche Diagnostic, Vifor Pharma, AstraZeneca, Novartis, Amgen, Janssen Research & Development LLC, Menarini, Boehringer Ingelheim, Abbott Diagnostics, Corvia, Stealth BioTherapeutics, Novo Nordisk, JanaCare, Biofourmis, Darma, Applied Therapeutics, MyoKardia, Cytokinetics, WebMD Global LLC, Radcliffe Group Ltd, and Corpus; and serves as cofounder and nonexecutive director of eKo.ai. S. Schnaidt, Dr Ofstad, Dr Brueckmann, and Dr Jamal are employees of Boehringer Ingelheim. Dr Bocchi reports receiving consulting fees from Servier and Astra-Zeneca; subsidized travel/hotel/registration fees from Servier and Baldacci; membership in steering committees for Servier and Novartis; contracted research from Jansen, Bayer/Merck, Astra-Zeneca, Boehringer, and Ingelheim; and honoraria from Servier, Novartis, and Astra-Zeneca. Dr Ponikowski reports personal fees from Boehringer Ingelheim, Astra Zeneca, Servier, BMS, Amgen, Novartis, Merck, Pfizer, and Berlin Chemie, and grants and personal fees from Vifor Pharma. Dr Perrone serves on advisory boards and receives personal fees from Laboratorios Ferrer, Abbott–St Jude, Novartis, and Laboratorios Bago. Dr Januzzi reports grant support, consulting income, and participation in clinical end point committees/data safety monitoring boards from Janssen; participation in clinical end point committees/data safety monitoring boards from Boehringer Ingelheim; grant support from Novartis, Innolife, Applied Therapeutics, and Siemens Diagnostics; and consultancy fees from Novartis, Roche Diagnostics, and Abbott Diagnostics. Dr Verma holds a Tier 1 Canada Research Chair in Cardiovascular Surgery; reports receiving research grants and/or speaking honoraria from Amarin, Amgen, AstraZeneca, Bayer, Boehringer Ingelheim, Bristol-Myers Squibb, Eli Lilly, EOCI Pharmacomm Ltd, HLS Therapeutics, Janssen, Merck, Novartis, Novo Nordisk, Sanofi, Sun Pharmaceuticals, PhaseBio, and the Toronto Knowledge Translation Working Group; is a member of the scientific excellence committee of EMPEROR-Reduced and served as a national lead investigator of the DAPA-HF trial and EMPEROR-Reduced; and is the President of the Canadian Medical and Surgical Knowledge Translation Research Group, a federally incorporated not-for-profit physician organization. Dr Böhm reports fees from Amgen, AstraZeneca, Bayer, Boehringer Ingelheim, Cytokinetics, Servier, Medtronic, ReCor, Vifor, Novartis, and Abbott; and is supported by the Deutsche Forschungsgemeinschaft (grant TTR 219, S-01). Dr Ferreira is a consultant for Boehringer Ingelheim. Dr Pocock is a consultant for Boehringer Ingelheim. Dr Zannad has recently received steering committee or advisory board fees from Amgen, AstraZeneca, Bayer, Boehringer Ingelheim, Boston Scientific, Cardior, CVRx, Janssen, Livanova, Merck, Mundipharma, Novartis, Novo Nordisk, and Vifor Fresenius. Dr Packer reports personal fees from Boehringer Ingelheim during the conduct of the study and personal fees from AbbVie, Akcea, Amarin, AstraZeneca, Amgen, Boehringer Ingelheim, Cardiorentis, Daiichi Sankyo, Johnson & Johnson, Lilly, Novartis, Pfizer, Relypsa, Sanofi, Synthetic Biologics, Theravance, and NovoNordisk, outside the submitted work.
Figures
Comment in
-
Diamonds in the Rough: The Incredible-but-True Story of Sodium Glucose Cotransporter 2 Inhibitors in Treatment of Heart Failure.Circulation. 2021 Jan 26;143(4):350-353. doi: 10.1161/CIRCULATIONAHA.120.052446. Epub 2021 Jan 25. Circulation. 2021. PMID: 33493031 No abstract available.
References
-
- Zelniker TA, Wiviott SD, Raz I, Im K, Goodrich EL, Bonaca MP, Mosenzon O, Kato ET, Cahn A, Furtado RHM, et al. SGLT2 inhibitors for primary and secondary prevention of cardiovascular and renal outcomes in type 2 diabetes: a systematic review and meta-analysis of cardiovascular outcome trials. Lancet. 2019; 393:31–39. doi: 10.1016/S0140-6736(18)32590-X - PubMed
-
- Butler J, Handelsman Y, Bakris G, Verma S. Use of sodium-glucose co-transporter-2 inhibitors in patients with and without type 2 diabetes: implications for incident and prevalent heart failure. Eur J Heart Fail. 2020; 22:604–617. doi: 10.1002/ejhf.1708 - PubMed
-
- Neuen BL, Young T, Heerspink HJL, Neal B, Perkovic V, Billot L, Mahaffey KW, Charytan DM, Wheeler DC, Arnott C, et al. SGLT2 inhibitors for the prevention of kidney failure in patients with type 2 diabetes: a systematic review and meta-analysis. Lancet Diabetes Endocrinol. 2019; 7:845–854. doi: 10.1016/S2213-8587(19)30256-6 - PubMed
-
- Packer M. SGLT2 inhibitors produce cardiorenal benefits by promoting adaptive cellular reprogramming to induce a state of fasting mimicry: a paradigm shift in understanding their mechanism of action. Diabetes Care. 2020; 43:508–511. doi: 10.2337/dci19-0074 - PubMed
-
- McMurray JJV, Solomon SD, Inzucchi SE, Køber L, Kosiborod MN, Martinez FA, Ponikowski P, Sabatine MS, Anand IS, Bělohlávek J, et al. DAPA-HF Trial Committees and Investigators. Dapagliflozin in patients with heart failure and reduced ejection fraction. N Engl J Med. 2019; 381:1995–2008. doi: 10.1056/NEJMoa1911303 - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
