

Automated Identification of Adults at Risk for In-Hospital Clinical Deterioration
- PMID: 33176085
- PMCID: PMC7787261
- DOI: 10.1056/NEJMsa2001090
Automated Identification of Adults at Risk for In-Hospital Clinical Deterioration
Abstract
Background: Hospitalized adults whose condition deteriorates while they are in wards (outside the intensive care unit [ICU]) have considerable morbidity and mortality. Early identification of patients at risk for clinical deterioration has relied on manually calculated scores. Outcomes after an automated detection of impending clinical deterioration have not been widely reported.
Methods: On the basis of a validated model that uses information from electronic medical records to identify hospitalized patients at high risk for clinical deterioration (which permits automated, real-time risk-score calculation), we developed an intervention program involving remote monitoring by nurses who reviewed records of patients who had been identified as being at high risk; results of this monitoring were then communicated to rapid-response teams at hospitals. We compared outcomes (including the primary outcome, mortality within 30 days after an alert) among hospitalized patients (excluding those in the ICU) whose condition reached the alert threshold at hospitals where the system was operational (intervention sites, where alerts led to a clinical response) with outcomes among patients at hospitals where the system had not yet been deployed (comparison sites, where a patient's condition would have triggered a clinical response after an alert had the system been operational). Multivariate analyses adjusted for demographic characteristics, severity of illness, and burden of coexisting conditions.
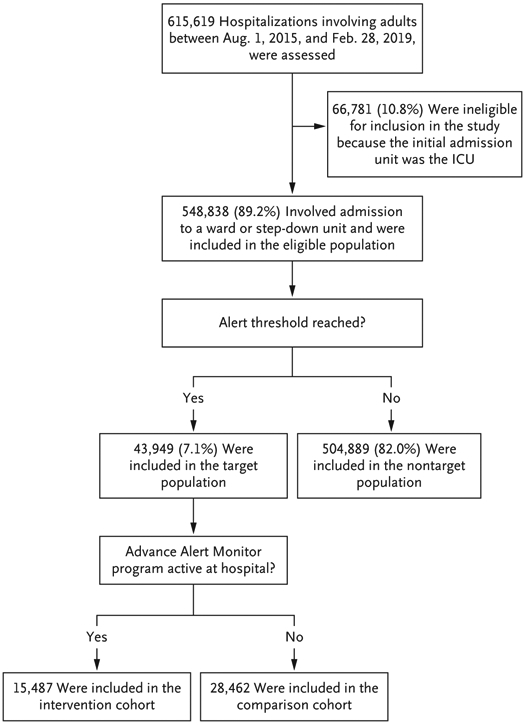
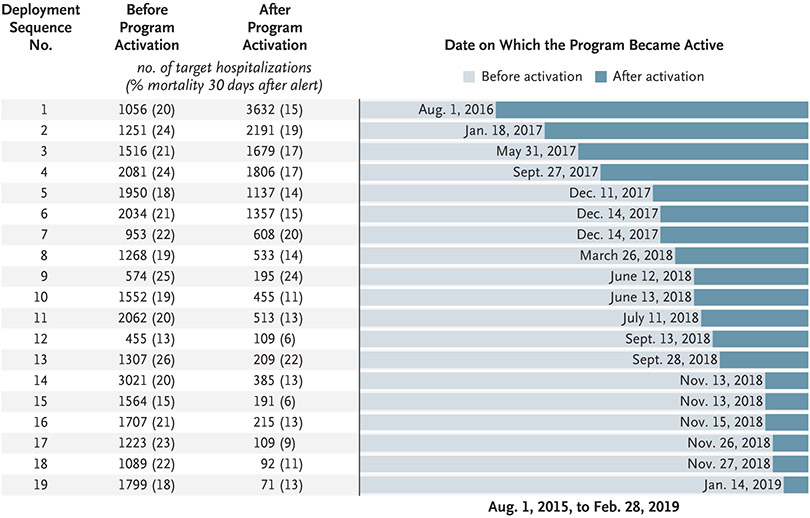
Results: The program was deployed in a staggered fashion at 19 hospitals between August 1, 2016, and February 28, 2019. We identified 548,838 non-ICU hospitalizations involving 326,816 patients. A total of 43,949 hospitalizations (involving 35,669 patients) involved a patient whose condition reached the alert threshold; 15,487 hospitalizations were included in the intervention cohort, and 28,462 hospitalizations in the comparison cohort. Mortality within 30 days after an alert was lower in the intervention cohort than in the comparison cohort (adjusted relative risk, 0.84, 95% confidence interval, 0.78 to 0.90; P<0.001).
Conclusions: The use of an automated predictive model to identify high-risk patients for whom interventions by rapid-response teams could be implemented was associated with decreased mortality. (Funded by the Gordon and Betty Moore Foundation and others.).
Copyright © 2020 Massachusetts Medical Society.
Figures
Comment in
-
Automated Identification of Adults at Risk for In-Hospital Clinical Deterioration.N Engl J Med. 2021 Feb 4;384(5):485. doi: 10.1056/NEJMc2034836. N Engl J Med. 2021. PMID: 33534985 No abstract available.
-
Automated Identification of Adults at Risk for In-Hospital Clinical Deterioration.N Engl J Med. 2021 Feb 4;384(5):485-486. doi: 10.1056/NEJMc2034836. N Engl J Med. 2021. PMID: 33534986 No abstract available.
-
The opportunity to use electronic health record data for real-time improvement of inpatient care.Surgery. 2021 Sep;170(3):978. doi: 10.1016/j.surg.2021.01.032. Epub 2021 Mar 7. Surgery. 2021. PMID: 33691938 No abstract available.
References
-
- Bapoje SR, Gaudiani JL, Narayanan V, Albert RK. Unplanned transfers to a medical intensive care unit: causes and relationship to preventable errors in care. J Hosp Med 2011;6:68–72. - PubMed
-
- Escobar GJ, Greene JD, Gardner MN, Marelich GP, Quick B, Kipnis P. Intrahospital transfers to a higher level of care: contribution to total hospital and intensive care unit (ICU) mortality and length of stay (LOS). J Hosp Med 2011;6:74–80. - PubMed
-
- Delgado MK, Liu V, Pines JM, Kipnis P, Gardner MN, Escobar GJ. Risk factors for unplanned transfer to intensive care within 24 hours of admission from the emergency department in an integrated healthcare system. J Hosp Med 2013;8:13–9. - PubMed
-
- Liu V, Kipnis P, Rizk NW, Escobar GJ. Adverse outcomes associated with delayed intensive care unit transfers in an integrated healthcare system. J Hosp Med 2012;7:224–30. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources