

Determinants of Value in Coronary Artery Bypass Grafting
- PMID: 33176461
- PMCID: PMC8041058
- DOI: 10.1161/CIRCOUTCOMES.119.006374
Determinants of Value in Coronary Artery Bypass Grafting
Abstract
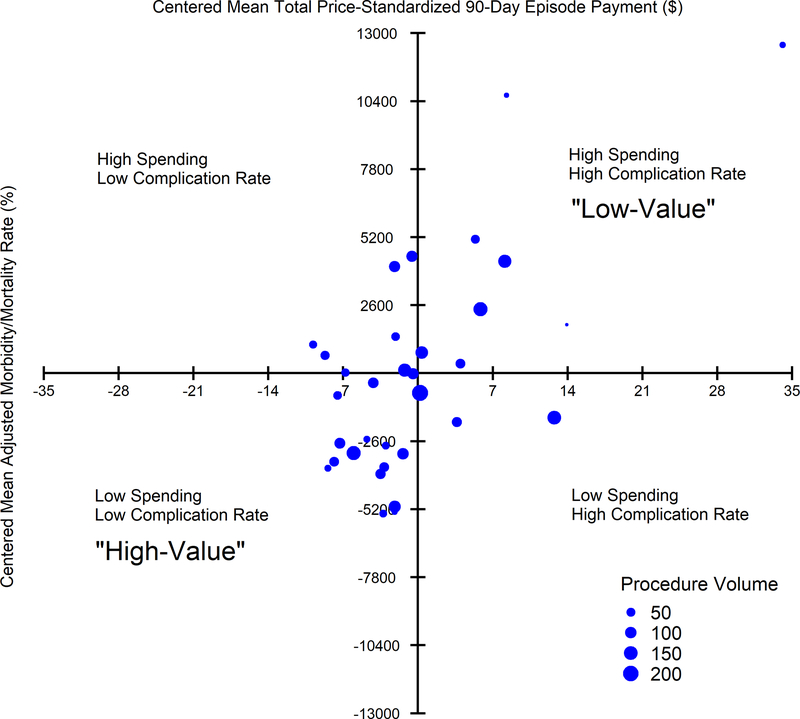
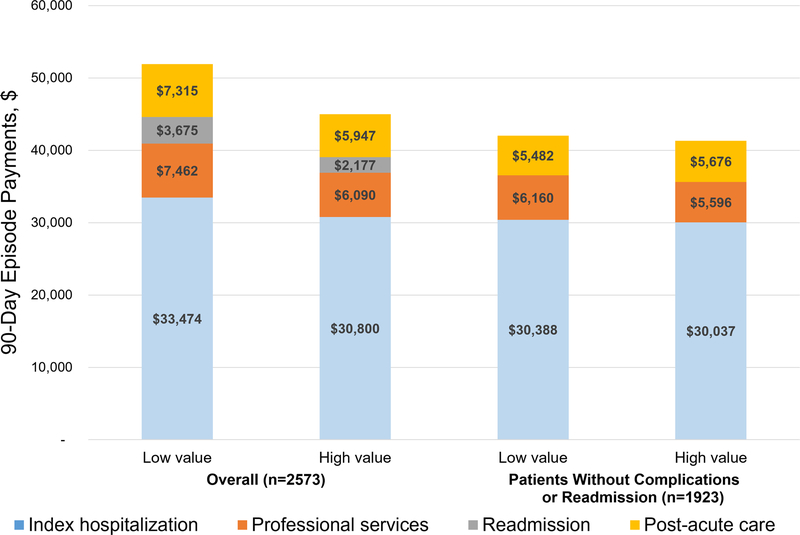
Background Over 180 000 coronary artery bypass grafting (CABG) procedures are performed annually, accounting for $7 to $10 billion in episode expenditures. Assessing tradeoffs between spending and quality contributing to value during 90-day episodes has not been conducted but is essential for success in bundled reimbursement models. We, therefore, identified determinants of variability in hospital 90-day episode value for CABG. Methods Medicare and private payor admissions for isolated CABG from 2014 to 2016 were retrospectively linked to clinical registry data for 33 nonfederal hospitals in Michigan. Hospital composite risk-adjusted complication rates (≥1 National Quality Forum-endorsed, Society of Thoracic Surgeons measure: deep sternal wound infection, renal failure, prolonged ventilation >24 hours, stroke, re-exploration, and operative mortality) and 90-day risk-adjusted, price-standardized episode payments were used to categorize hospitals by value by defining the intersection between complications and spending. Results Among 2573 total patients, those at low- versus high-value hospitals had a higher percentage of prolonged length of stay >14 days (9.3% versus 2.4%, P=0.006), prolonged ventilation (17.6% versus 4.8%, P<0.001), and operative mortality (4.8% versus 0.6%, P=0.001). Mean total episode payments were $51 509 at low-compared with $45 526 at high-value hospitals (P<0.001), driven by higher readmission ($3675 versus $2177, P=0.005), professional ($7462 versus $6090, P<0.001), postacute care ($7315 versus $5947, P=0.031), and index hospitalization payments ($33 474 versus $30 800, P<0.001). Among patients not experiencing a complication or 30-day readmission (1923/2573, 74.7%), low-value hospitals had higher inpatient evaluation and management payments ($1405 versus $752, P<0.001) and higher utilization of inpatient rehabilitation (7% versus 2%, P<0.001), but lower utilization of home health (66% versus 73%, P=0.016) and emergency department services (13% versus 17%, P=0.034). Conclusions To succeed in emerging bundled reimbursement programs for CABG, hospitals and physicians should identify strategies to minimize complications while optimizing inpatient evaluation and management spending and use of inpatient rehabilitation, home health, and emergency department services.
Keywords: coronary artery bypass; hospitalization; inpatient; length of stay; pneumonia.
Figures
References
-
- D’Agostino RS, Jacobs JP, Badhwar V, Fernandez FG, Paone G, Wormuth DW, Shahian DM. The Society of Thoracic Surgeons Adult Cardiac Surgery Database: 2019 Update on Outcomes and Quality. Ann Thorac Surg. 2019;107:24–32. - PubMed
-
- Thompson MP, Cabrera L, Strobel RJ, Harrington SD, Zhang M, Wu X, Prager RL, Likosky DS. Association Between Postoperative Pneumonia and 90-Day Episode Payments and Outcomes Among Medicare Beneficiaries Undergoing Cardiac Surgery. Circ Cardiovasc Qual Outcomes. 2018;11:e004818. - PubMed
-
- Ghaferi AA, Birkmeyer JD, Dimick JB. Variation in hospital mortality associated with inpatient surgery. N Engl J Med. 2009;361:1368–1375. - PubMed
-
- Shih T, Zhang M, Kommareddi M, Boeve TJ, Harrington SD, Holmes RJ, Roth G, Theurer PF, Prager RL, Likosky DS; Michigan Society of Thoracic and Cardiovascular Surgeons Quality Collaborative. Center-Level Variation in Infection Rates After Coronary Artery Bypass Grafting. Circ Cardiovasc Qual Outcomes. 2014;7:567–573. - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
