

Clinical management of sickle cell liver disease in children and young adults
- PMID: 33177052
- PMCID: PMC7610372
- DOI: 10.1136/archdischild-2020-319778
Clinical management of sickle cell liver disease in children and young adults
Abstract
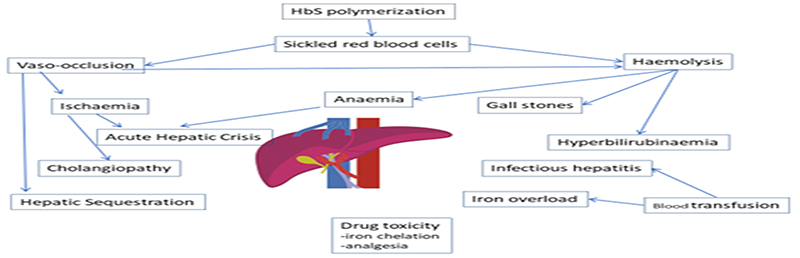
Liver involvement in sickle cell disease (SCD) is often referred to as sickle cell hepatopathy (SCH) and is a complication of SCD which may be associated with significant mortality. This review is based on a round-table workshop between paediatric and adult hepatologists and haematologists and review of the literature. The discussion was prompted by the lack of substantial data and guidance in managing these sometimes very challenging cases. This review provides a structured approach for the diagnosis and management of SCH in children and young adults. The term SCH describes any hepatobiliary dysfunction in the context of SCD. Diagnosis and management of biliary complications, acute hepatic crisis, acute hepatic sequestration and other manifestations of SCH are discussed, as well as the role of liver transplantation and haemopoietic stem cell transplantation in the management of SCH.
Keywords: adolescent health; gastroenterology; jaundice.
© Author(s) (or their employer(s)) 2021. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: EK, FL, EF, MDa, NHe, SH, MS, FM, VB, AS, AV, MV, BI, ED, NHa, TG, JH, MDe, MS and AD have nothing to disclose. DR is on advisory boards of Novartis and DSMB of AstraZeneca outside the submitted work. GG reports personal fees from Alexion Pharmaceuticals outside the submitted work. SC reports personal fees from Novartis outside the submitted work. VB reports personal fees from Bluebirdbio and from Addmedica, outside the submitted work.
Figures


References
-
- Hamideh D, Alvarez O. Sickle cell disease related mortality in the United States (1999-2009) Pediatr Blood Cancer. 2013;60(9):1482–6. - PubMed
-
- Alkindi SY, Pathare A, Al Zadjali S, et al. Serum Total Bilirubin, not Cholelithiasis, is Influenced by UGT1A1 Polymorphism, Alpha Thalassemia and beta(s) Haplotype: First Report on Comparison between Arab-Indian and African beta(s) Genes. Mediterr J Hematol Infect Dis. 2015;7(1):e2015060. - PMC - PubMed
-
- Walker TM, Hambleton IR, Serjeant GR. Gallstones in sickle cell disease: observations from The Jamaican Cohort study. J Pediatr. 2000;136(1):80–5. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous