

Intraoperative Hypotension Is Associated With Adverse Clinical Outcomes After Noncardiac Surgery
- PMID: 33177322
- PMCID: PMC8115733
- DOI: 10.1213/ANE.0000000000005250
Intraoperative Hypotension Is Associated With Adverse Clinical Outcomes After Noncardiac Surgery
Abstract
Background: Intraoperative hypotension (IOH) occurs frequently during surgery and may be associated with organ ischemia; however, few multicenter studies report data regarding its associations with adverse postoperative outcomes across varying hemodynamic thresholds. Additionally, no study has evaluated the association between IOH exposure and adverse outcomes among patients by various age groups.
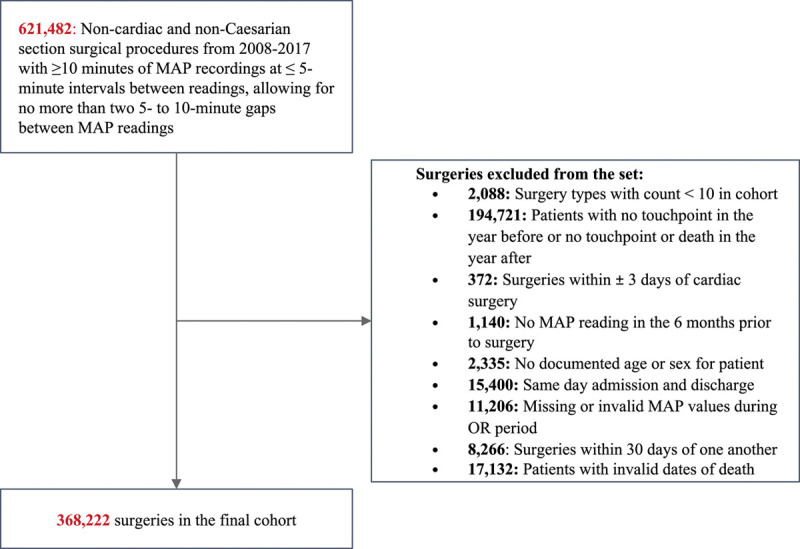
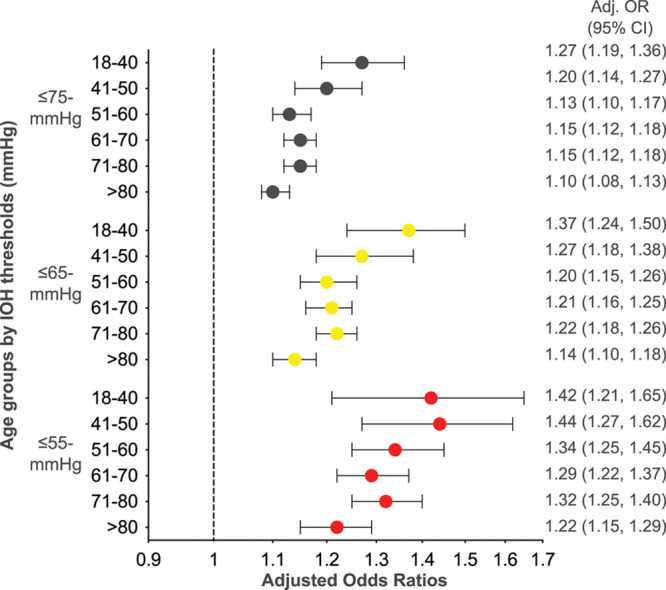
Methods: A multicenter retrospective cohort study was conducted between 2008 and 2017 using intraoperative blood pressure data from the US electronic health records database to examine postoperative outcomes. IOH was assessed in 368,222 noncardiac surgical procedures using 5 methods: (a) absolute maximum decrease in mean arterial pressure (MAP) during surgery, (b) time under each absolute threshold, (c) total area under each threshold, (d) time-weighted average MAP under each threshold, and (e) cumulative time under the prespecified relative MAP thresholds. MAP thresholds were defined by absolute limits (≤75, ≤65, ≤55 mm Hg) and by relative limits (20% and 40% lower than baseline). The primary outcome was major adverse cardiac or cerebrovascular events; secondary outcomes were all-cause 30- and 90-day mortality, 30-day acute myocardial injury, and 30-day acute ischemic stroke. Residual confounding was minimized by controlling for observable patient and surgical factors. In addition, we stratified patients into age subgroups (18-40, 41-50, 51-60, 61-70, 71-80, >80) to investigate how the association between hypotension and the likelihood of major adverse cardiac or cerebrovascular events and acute kidney injury differs in these age subgroups.
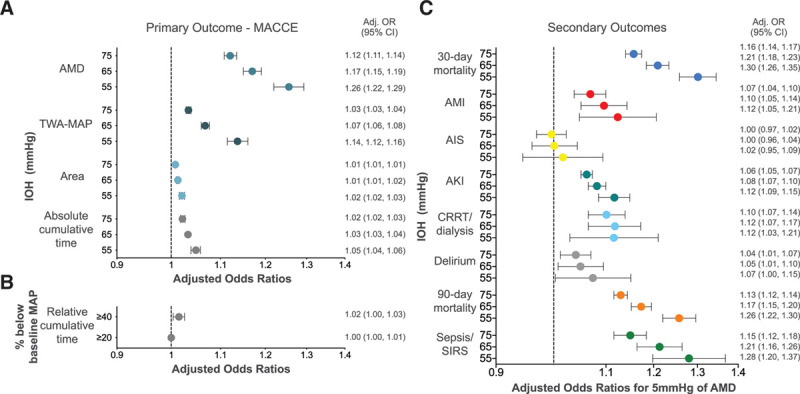
Results: IOH was common with at least 1 reading of MAP ≤75 mm Hg occurring in 39.5% (145,743) of cases; ≤65 mm Hg in 19.3% (70,938) of cases, and ≤55 mm Hg in 7.5% (27,473) of cases. IOH was significantly associated with the primary outcome for all age groups. For an absolute maximum decrease, the estimated odds of a major adverse cardiac or cerebrovascular events in the 30-day postsurgery was increased by 12% (95% confidence interval [CI], 11-14) for ≤75 mm Hg; 17.0% (95% CI, 15-19) for ≤65 mm Hg; and by 26.0% (95% CI, 22-29) for ≤55 mm Hg.
Conclusions: IOH during noncardiac surgery is common and associated with increased 30-day major adverse cardiac or cerebrovascular events. This observation is magnified with increasing hypotension severity. The potentially avoidable nature of the hazard, and the extent of the exposed population, makes hypotension in the operating room a serious public health issue that should not be ignored for any age group.
Copyright © 2020 The Author(s). Published by Wolters Kluwer Health, Inc. on behalf of the International Anesthesia Research Society.
Conflict of interest statement
Conflicts of Interest: See Disclosures at the end of the article.
Figures
Comment in
-
Just One?Anesth Analg. 2021 Jul 1;133(1):e3. doi: 10.1213/ANE.0000000000005436. Anesth Analg. 2021. PMID: 34127595 No abstract available.
References
-
- Bijker JB, van Klei WA, Kappen TH, van Wolfswinkel L, Moons KG, Kalkman CJ. Incidence of intraoperative hypotension as a function of the chosen definition: literature definitions applied to a retrospective cohort using automated data collection. Anesthesiology. 2007;107:213–220. - PubMed
-
- Seeling M, Papkalla N, Radtke F, Franck M, Spies C. Incidence of intraoperative hypotension during anaesthesia varies greatly with the chosen definition: 1AP1-5. Eur J Anaesthesiol. 2008;25:8.
-
- Monk TG, Bronsert MR, Henderson WG, et al. Association between intraoperative hypotension and hypertension and 30-day postoperative mortality in noncardiac surgery. Anesthesiology. 2015;123:307–319. - PubMed
-
- Wesselink EM, Kappen TH, Torn HM, Slooter AJC, van Klei WA. Intraoperative hypotension and the risk of postoperative adverse outcomes: a systematic review. Br J Anaesth. 2018;121:706–721. - PubMed
