

Association Between Plasma Lipoprotein-Associated Phospholipase A2 and Plaque Vulnerability in TIA Patients With Unilateral Middle Cerebral Artery Stenosis
- PMID: 33178116
- PMCID: PMC7596647
- DOI: 10.3389/fneur.2020.574036
Association Between Plasma Lipoprotein-Associated Phospholipase A2 and Plaque Vulnerability in TIA Patients With Unilateral Middle Cerebral Artery Stenosis
Abstract
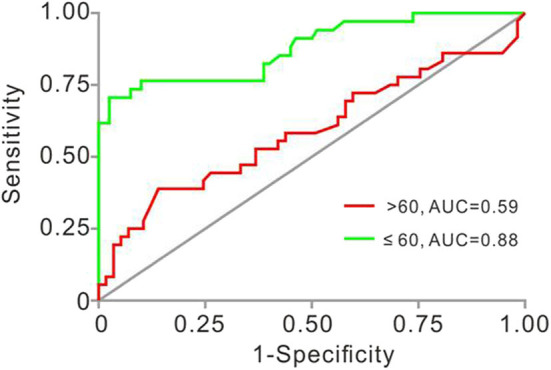
Background: Plasma lipoprotein-associated phospholipase A2 (Lp-PLA2) has emerged as a novel biomarker for coronary atherosclerosis. However, the association between Lp-PLA2 and plaque vulnerability in atherosclerosis of cervicocerebral arteries remains poorly defined, especially for intracranial atherosclerotic stenosis (ICAS). We aimed to investigate the association between Lp-PLA2 and plaque vulnerability in transient ischemic attack (TIA) patients with unilateral middle cerebral artery stenoses (MCAs). Methods: In this study, a total of 207 patients were enrolled from April 2017 to April 2020. Clinical data were collected, and MCA plaques were examined with high-resolution magnetic resonance imaging (HRMRI). Baseline characteristics of patients were collected during hospitalization. Statistical comparisons were performed using Pearson's chi-squared test, Mann-Whitney U test, and the Breslow-Day/Tarone's test for the determination of heterogeneity in different age strata. Multivariate binary logistic analysis was used to investigate the potential independent predictors that were highly correlated to plaque vulnerability. Results: The results showed that a high Lp-PLA2 level (>221 ng/ml) was associated with plaque vulnerability in TIA patients with unilateral MCAs. High Lp-PLA2 was independently associated with plaque vulnerability in patients ≤ 60 years old [multivariate adjusted odds ratio (OR) = 9.854; 95% CI, 2.458-39.501] but not in patients >60 years old (multivariate adjusted OR = 1.901; 95% CI, 0.640-5.650). Predictors of plaque vulnerability in different age strata were also different. Conclusion: Lp-PLA2 levels may be correlated to plaque vulnerability in TIA patients with unilateral MCAs and might be a diagnostic biomarker for plaque vulnerability in this kind of patients, especially for ones aged ≤ 60 years old.
Keywords: HRMRI; ICAs; Lp-PLA2; middle cerebral artery; transient ischemic attack.
Copyright © 2020 Qin, Qian, Luo, Li, Wang, Jiang, Zhang, Liu, Xiao, Zhang, Diao and Zhao.
Figures
Similar articles
-
Combined Assessment of Elevated Plasma Lipoprotein-Associated Phospholipase A2 and Plaque Enhancement Improved Accuracy in the Risk of Acute Ischemic Stroke in Patients with Intracranial Artery Stenosis.J Stroke Cerebrovasc Dis. 2021 Dec;30(12):106103. doi: 10.1016/j.jstrokecerebrovasdis.2021.106103. Epub 2021 Sep 27. J Stroke Cerebrovasc Dis. 2021. PMID: 34587576
-
Serum lipoprotein-associated phospholipase A2 predicts the formation of carotid artery plaque and its vulnerability in anterior circulation cerebral infarction.Clin Neurol Neurosurg. 2017 Sep;160:40-45. doi: 10.1016/j.clineuro.2017.06.007. Epub 2017 Jun 12. Clin Neurol Neurosurg. 2017. PMID: 28644968
-
Association of lipoprotein-associated phospholipase A2 mass with asymptomatic cerebral artery stenosis.J Cell Mol Med. 2018 Apr;22(4):2329-2336. doi: 10.1111/jcmm.13521. Epub 2018 Feb 9. J Cell Mol Med. 2018. PMID: 29424477 Free PMC article.
-
[Does Lp-PLA2 determination help predict atherosclerosis and cardiocerebrovascular disease?].Acta Med Croatica. 2010 Oct;64(4):237-45. Acta Med Croatica. 2010. PMID: 21688606 Review. Croatian.
-
[Lp-PLA2, a biomarker of vascular inflammation and vulnerability of atherosclerosis plaques].Ann Pharm Fr. 2016 May;74(3):190-7. doi: 10.1016/j.pharma.2015.09.002. Epub 2015 Oct 21. Ann Pharm Fr. 2016. PMID: 26499399 Review. French.
Cited by
-
A retrospective study of immunoglobulin E as a biomarker for the diagnosis of acute ischemic stroke with carotid atherosclerotic plaques.PeerJ. 2022 Oct 26;10:e14235. doi: 10.7717/peerj.14235. eCollection 2022. PeerJ. 2022. PMID: 36317119 Free PMC article.
-
The Value of Lp-PLA2 as a Biomarker for the Diagnosis of Plaque Stability in Atherosclerosis: A Meta-Analysis.Clin Appl Thromb Hemost. 2025 Jan-Dec;31:10760296251360015. doi: 10.1177/10760296251360015. Epub 2025 Aug 10. Clin Appl Thromb Hemost. 2025. PMID: 40785298 Free PMC article.
-
Lipoprotein-Associated Phospholipase A2 Is a Risk Factor for Patients With Parkinson's Disease.Front Neurosci. 2021 Apr 20;15:633022. doi: 10.3389/fnins.2021.633022. eCollection 2021. Front Neurosci. 2021. PMID: 33958981 Free PMC article.
-
Elevated Lipoprotein-Associated Phospholipase A2 Is Associated With Intracranial Atherosclerosis.Front Neurol. 2022 Jun 10;13:858302. doi: 10.3389/fneur.2022.858302. eCollection 2022. Front Neurol. 2022. PMID: 35756924 Free PMC article.
References
LinkOut - more resources
Full Text Sources
Miscellaneous