

A Longitudinal Study of Immune Cells in Severe COVID-19 Patients
- PMID: 33178207
- PMCID: PMC7597438
- DOI: 10.3389/fimmu.2020.580250
A Longitudinal Study of Immune Cells in Severe COVID-19 Patients
Abstract
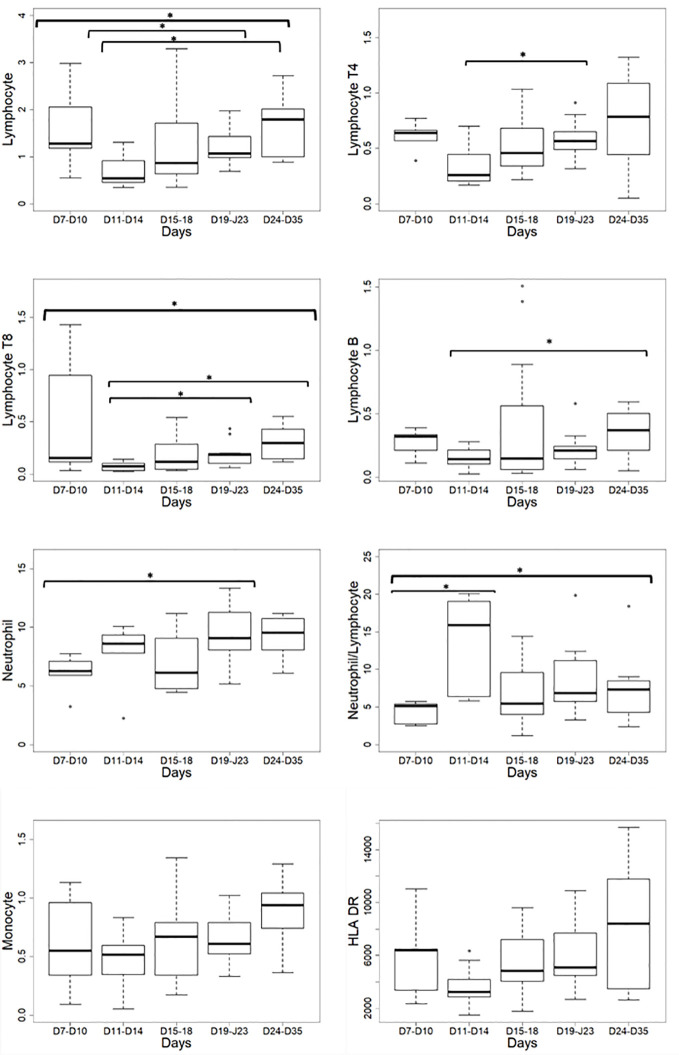
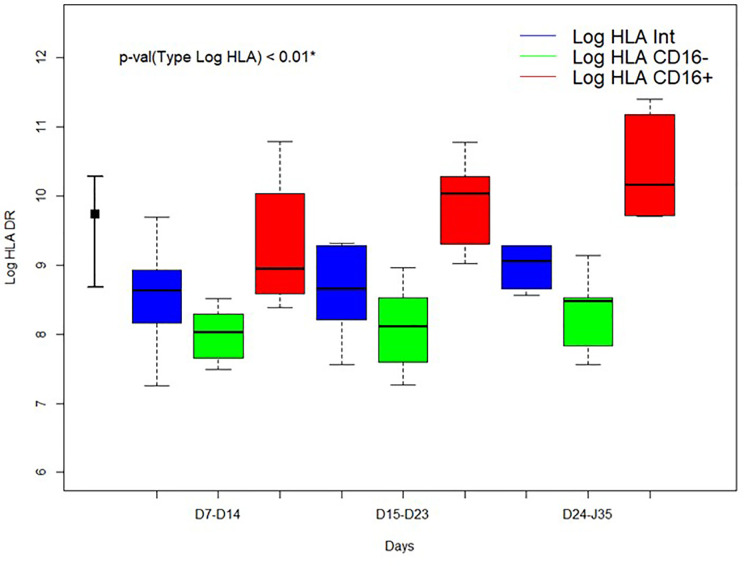
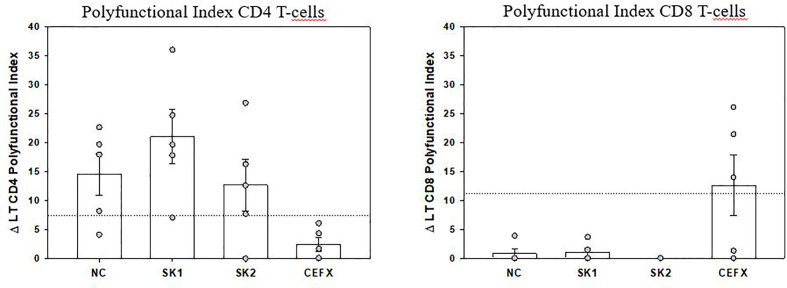
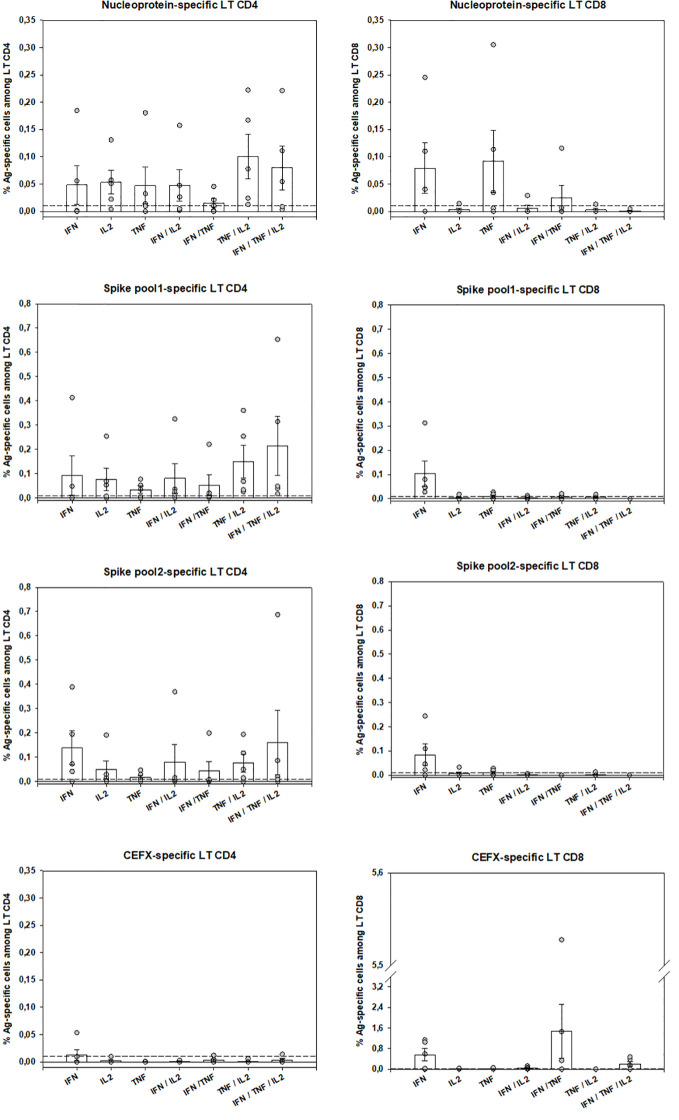
Little is known about the time-dependent immune responses in severe COVID-19. Data of 15 consecutive patients were sequentially recorded from intensive care unit admission. Lymphocyte subsets and total monocyte and subsets counts were monitored as well as the expression of HLA-DR. For 5 patients, SARS-CoV-2-specific T-cell polyfunctionality was assessed against Spike and Nucleoprotein SARS-CoV-2 peptides. Non-specific inflammation markers were increased in all patients. Median monocyte HLA-DR expression was below the 8,000 AB/C threshold defining acquired immunodepression. A "V" trend curve for lymphopenia, monocyte numbers, and HLA-DR expression was observed with a nadir between days 11 and 14 after symptoms' onset. Intermediate CD14++CD16+ monocytes increased early with a reduction in classic CD14++CD16- monocytes. Polyfunctional SARS-Cov-2-specific CD4 T-cells were present and functional, whereas virus-specific CD8 T-cells were less frequent and not efficient. We report a temporal variation of both innate and adaptive immunity in severe COVID-19 patients, helpful in guiding therapeutic decisions (e.g. anti-inflammatory vs. immunostimulatory ones). We describe a defect in virus-specific CD8 T-cells, a potential biomarker of clinical severity. These combined data also provide helpful knowledge for vaccine design.
Clinical trial registration: https://clinicaltrials.gov/, identifier NCT04386395.
Keywords: SARS-CoV-2; antigen-specific polyfunctional T-cells; immunity; intensive care unit; monocyte HLA-DR.
Copyright © 2020 Payen, Cravat, Maadadi, Didelot, Prosic, Dupuis, Losser and De Carvalho Bittencourt.
Figures
References
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous