

Managing the return to sport of the elite footballer following semimembranosus reconstruction
- PMID: 33178446
- PMCID: PMC7640780
- DOI: 10.1136/bmjsem-2020-000898
Managing the return to sport of the elite footballer following semimembranosus reconstruction
Abstract
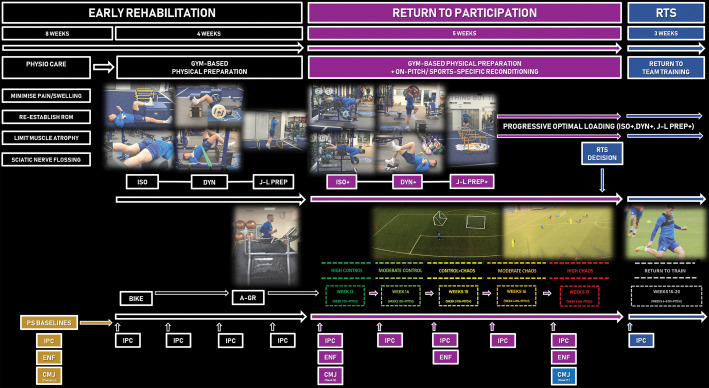
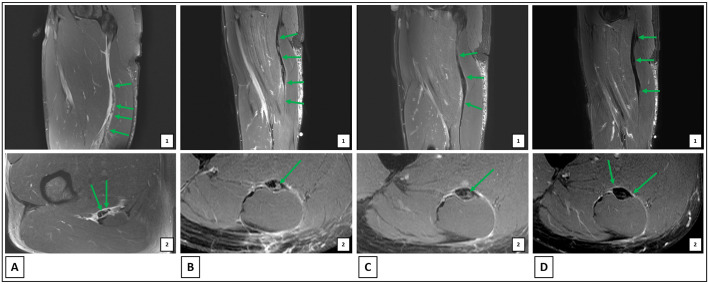
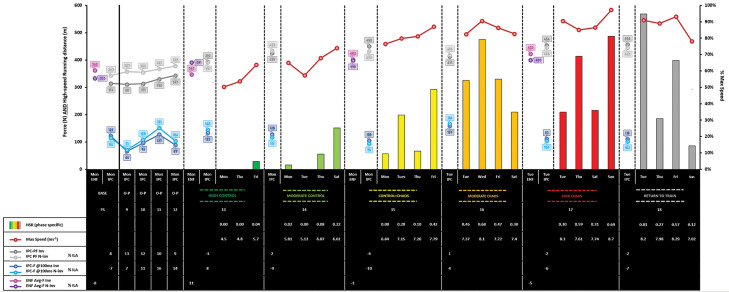
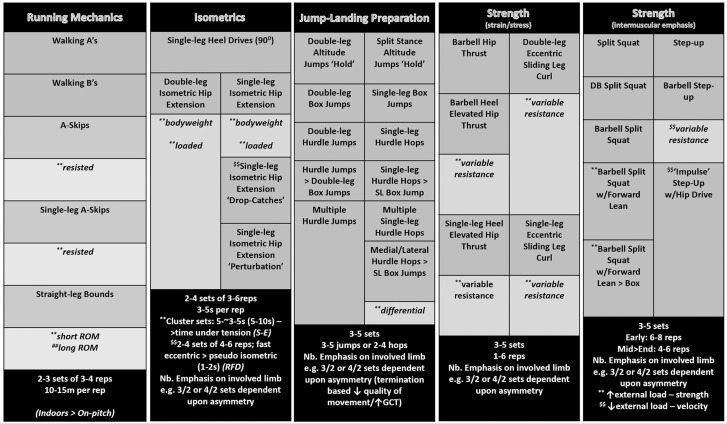
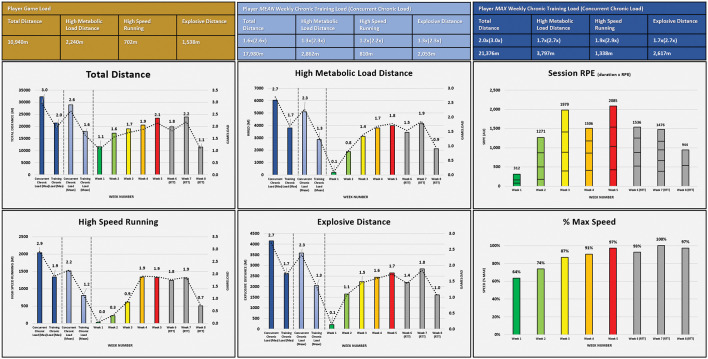
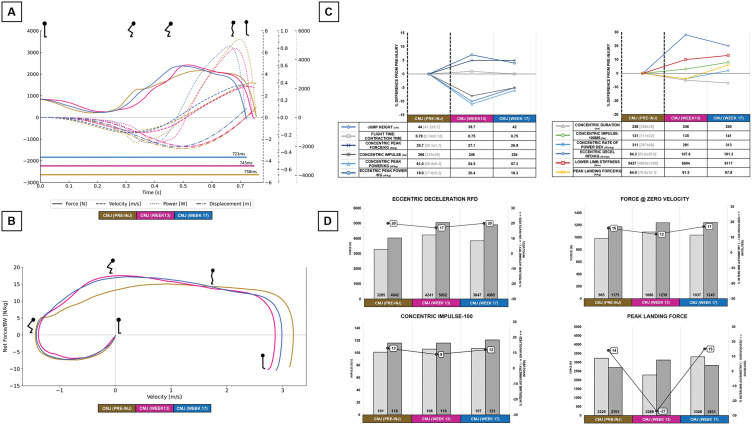
Hamstring strains are the most common injury in elite football and typically occur during high-speed running. Despite its important contribution to power production in the late swing phase, injury to the semimembranosus (SM) is less common than to the biceps femoris, but may involve the free tendon and depending on the degree of retraction, warrant surgical repair. Few case reports detail clinical reasoning, supported by objective data during rehabilitation in elite footballers, and none have described the return to sport (RTS) process following this type of hamstring injury. In this article, we outline the management and RTS of an English Premier League (EPL) footballer who suffered a high-grade SM proximal tendon tear during training. Due to the degree of retraction of the free tendon, the player underwent surgical reconstruction at the recommendation of an orthopaedic surgeon. Early physiotherapy care, nutritional support, on- and off-pitch injury-specific reconditioning and global athletic development are outlined, alongside strength and power diagnostic and global positioning systems data, assessment of pain, player feedback and MRI informed clinical reasoning and shared decision-making during the RTS process. 18 weeks post-surgery the player returned to team training, transferring to a new club 3 weeks later. 2.5 years post RTS, the player remains free of re-injury playing regularly in the EPL.
Keywords: Elite performance; Football; Hamstring; Rehabilitation; Surgery.
© Author(s) (or their employer(s)) 2020. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures

Similar articles
-
Return to sport and beyond following intramuscular tendon hamstring injury: A case report of an English Premier League football player.Phys Ther Sport. 2022 Jul;56:38-47. doi: 10.1016/j.ptsp.2022.05.013. Epub 2022 May 31. Phys Ther Sport. 2022. PMID: 35752044
-
Physical preparation and return to sport of the football player with a tibia-fibula fracture: applying the 'control-chaos continuum'.BMJ Open Sport Exerc Med. 2019 Oct 30;5(1):e000639. doi: 10.1136/bmjsem-2019-000639. eCollection 2019. BMJ Open Sport Exerc Med. 2019. PMID: 31749984 Free PMC article. Review.
-
Physical preparation and return to performance of an elite female football player following ACL reconstruction: a journey to the FIFA Women's World Cup.BMJ Open Sport Exerc Med. 2020 Dec 1;6(1):e000843. doi: 10.1136/bmjsem-2020-000843. eCollection 2020. BMJ Open Sport Exerc Med. 2020. PMID: 34422284 Free PMC article.
-
Association of the British Athletic Muscle Injury Classification and anatomic location with return to full training and reinjury following hamstring injury in elite football.BMJ Open Sport Exerc Med. 2021 May 10;7(2):e001010. doi: 10.1136/bmjsem-2020-001010. eCollection 2021. BMJ Open Sport Exerc Med. 2021. PMID: 34040793 Free PMC article.
-
Management of hamstring injuries: current concepts review.Bone Joint J. 2020 Oct;102-B(10):1281-1288. doi: 10.1302/0301-620X.102B10.BJJ-2020-1210.R1. Bone Joint J. 2020. PMID: 32993323 Review.
Cited by
-
Effectiveness of Conservative Interventions After Acute Hamstrings Injuries in Athletes: A Living Systematic Review.Sports Med. 2023 Mar;53(3):615-635. doi: 10.1007/s40279-022-01783-z. Epub 2023 Jan 9. Sports Med. 2023. PMID: 36622557
-
Complete Distal Rupture of the Rectus Femoris in an Elite Football Player: A Non-operative Treatment.Cureus. 2023 Sep 18;15(9):e45494. doi: 10.7759/cureus.45494. eCollection 2023 Sep. Cureus. 2023. PMID: 37859921 Free PMC article.
-
Consensus of Return-to-Play Criteria After Adductor Longus Injury in Professional Soccer.Sports (Basel). 2025 Apr 27;13(5):134. doi: 10.3390/sports13050134. Sports (Basel). 2025. PMID: 40423270 Free PMC article.
-
The Hamstrings: Anatomic and Physiologic Variations and Their Potential Relationships With Injury Risk.Front Physiol. 2021 Jul 7;12:694604. doi: 10.3389/fphys.2021.694604. eCollection 2021. Front Physiol. 2021. PMID: 34305648 Free PMC article. Review.
-
Return to Performance of a Soccer Player with an Adductor Longus Injury: A Case Report.Medicina (Kaunas). 2024 Dec 3;60(12):1998. doi: 10.3390/medicina60121998. Medicina (Kaunas). 2024. PMID: 39768878 Free PMC article.
References
LinkOut - more resources
Full Text Sources