

Metal artifact correction strategies in MRI-based attenuation correction in PET/MRI
- PMID: 33178954
- PMCID: PMC7592486
- DOI: 10.1259/bjro.20190033
Metal artifact correction strategies in MRI-based attenuation correction in PET/MRI
Abstract
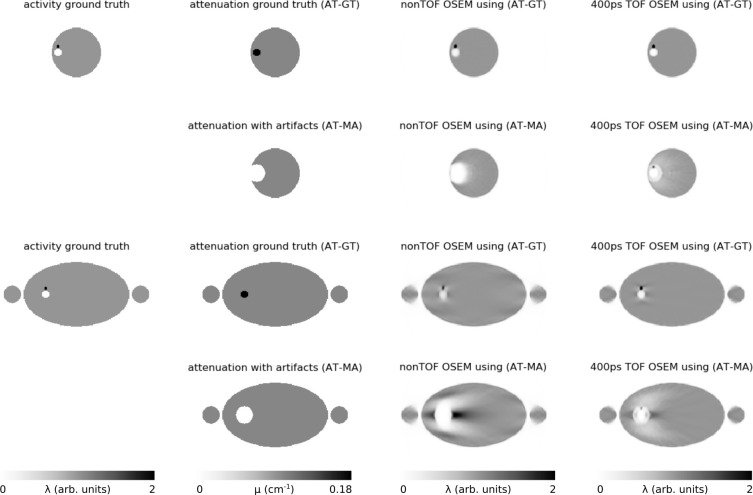
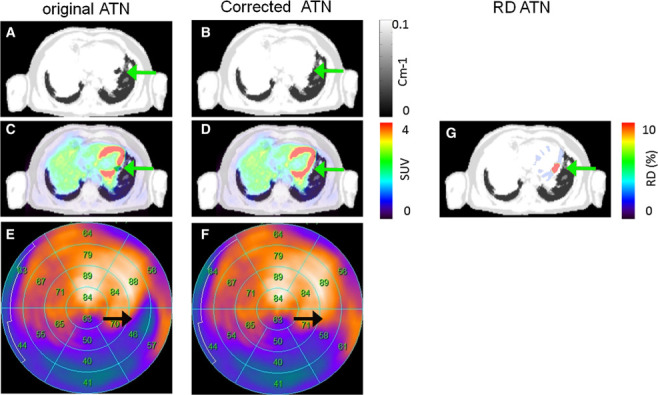
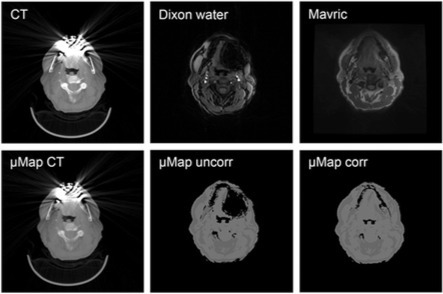
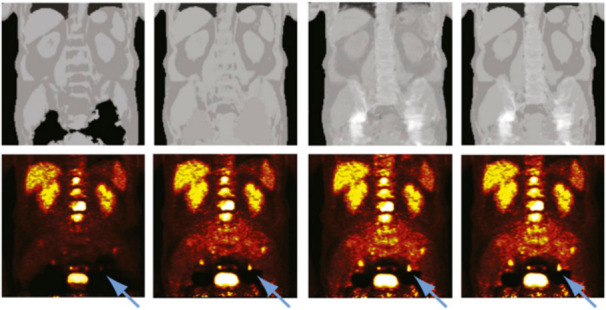
In hybrid positron emission tomography (PET) and MRI systems, attenuation correction for PET image reconstruction is commonly based on processing of dedicated MR images. The image quality of the latter is strongly affected by metallic objects inside the body, such as e.g. dental implants, endoprostheses, or surgical clips which all lead to substantial artifacts that propagate into MRI-based attenuation images. In this work, we review publications about metal artifact correction strategies in MRI-based attenuation correction in PET/MRI. Moreover, we also give an overview about publications investigating the impact of MRI-based attenuation correction metal artifacts on the reconstructed PET image quality and quantification.
© 2019 The Authors. Published by the British Institute of Radiology.
Figures




Similar articles
-
PET/MRI in the Presence of Metal Implants: Completion of the Attenuation Map from PET Emission Data.J Nucl Med. 2017 May;58(5):840-845. doi: 10.2967/jnumed.116.183343. Epub 2017 Jan 26. J Nucl Med. 2017. PMID: 28126884 Free PMC article.
-
Truncation compensation and metallic dental implant artefact reduction in PET/MRI attenuation correction using deep learning-based object completion.Phys Med Biol. 2020 Sep 25;65(19):195002. doi: 10.1088/1361-6560/abb02c. Phys Med Biol. 2020. PMID: 32976116
-
Does reducing CT artifacts from dental implants influence the PET interpretation in PET/CT studies of oral cancer and head and neck cancer?J Nucl Med. 2008 Jul;49(7):1047-52. doi: 10.2967/jnumed.107.049858. Epub 2008 Jun 13. J Nucl Med. 2008. PMID: 18552154
-
Vision 20/20: Magnetic resonance imaging-guided attenuation correction in PET/MRI: Challenges, solutions, and opportunities.Med Phys. 2016 Mar;43(3):1130-55. doi: 10.1118/1.4941014. Med Phys. 2016. PMID: 26936700 Review.
-
X-ray-based attenuation correction for positron emission tomography/computed tomography scanners.Semin Nucl Med. 2003 Jul;33(3):166-79. doi: 10.1053/snuc.2003.127307. Semin Nucl Med. 2003. PMID: 12931319 Review.
Cited by
-
Validation of PET/MRI attenuation correction methodology in the study of brain tumours.BMC Med Imaging. 2020 Nov 25;20(1):126. doi: 10.1186/s12880-020-00526-8. BMC Med Imaging. 2020. PMID: 33238917 Free PMC article.
-
Application of PET/MRI in Gynecologic Malignancies.Cancers (Basel). 2024 Apr 12;16(8):1478. doi: 10.3390/cancers16081478. Cancers (Basel). 2024. PMID: 38672560 Free PMC article. Review.
-
Attenuation correction for PET/MRI to measure tracer activity surrounding total knee arthroplasty.Eur J Hybrid Imaging. 2022 Nov 7;6(1):31. doi: 10.1186/s41824-022-00152-3. Eur J Hybrid Imaging. 2022. PMID: 36336748 Free PMC article.
-
Deep learning applications for quantitative and qualitative PET in PET/MR: technical and clinical unmet needs.MAGMA. 2024 Aug;37(4):749-763. doi: 10.1007/s10334-024-01199-y. Epub 2024 Aug 21. MAGMA. 2024. PMID: 39167304 Review.
-
Independent attenuation correction of whole body [18F]FDG-PET using a deep learning approach with Generative Adversarial Networks.EJNMMI Res. 2020 May 24;10(1):53. doi: 10.1186/s13550-020-00644-y. EJNMMI Res. 2020. PMID: 32449036 Free PMC article.
References
-
- Keereman V, Mollet P, Berker Y, Schulz V, Vandenberghe S. Challenges and current methods for attenuation correction in PET/MR. Magnetic Resonance Materials in Physics . Biology and Medicine 2013; 26: 81–98. - PubMed
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
