

Pitfalls in diagnosis of infiltrative lung disease by CT
- PMID: 33178955
- PMCID: PMC7592491
- DOI: 10.1259/bjro.20190036
Pitfalls in diagnosis of infiltrative lung disease by CT
Abstract
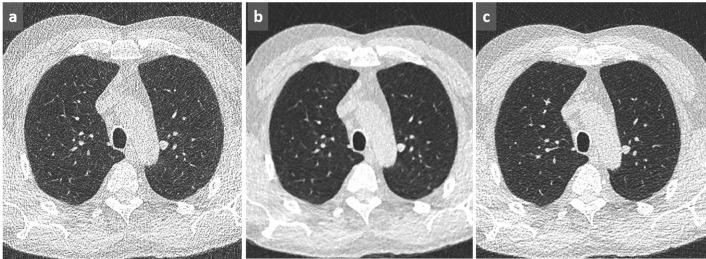
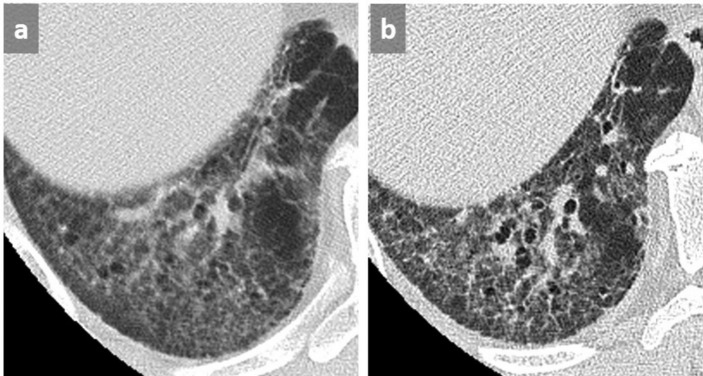
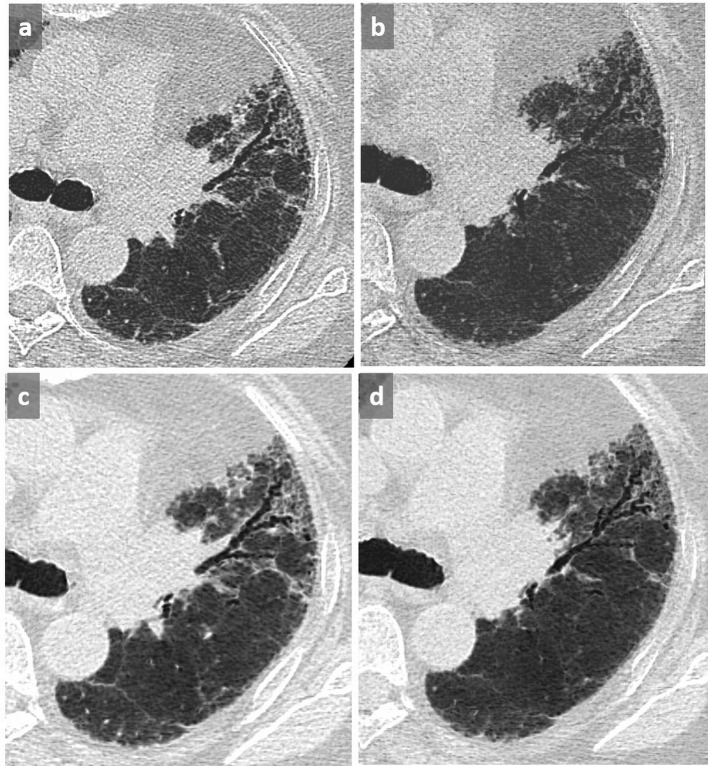
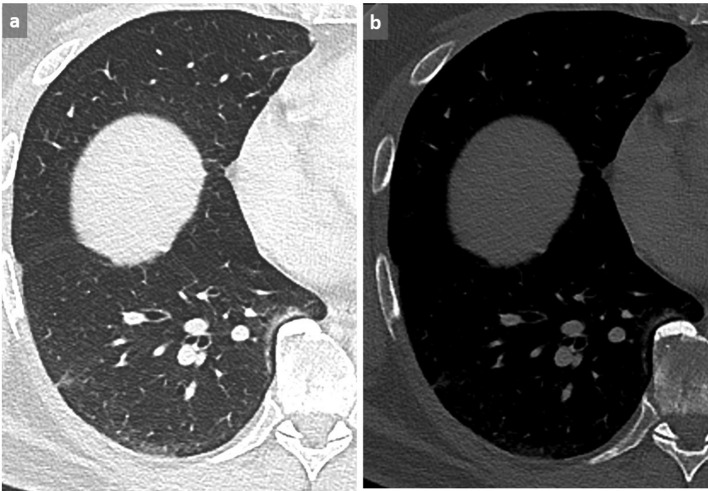
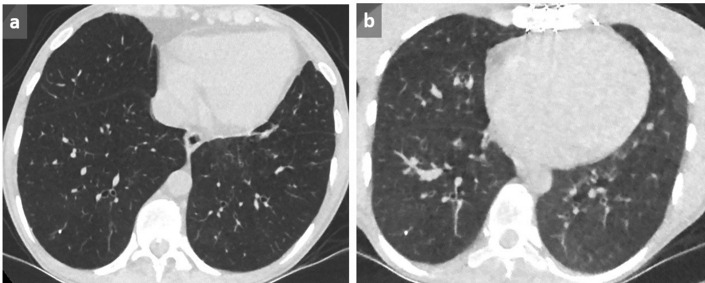
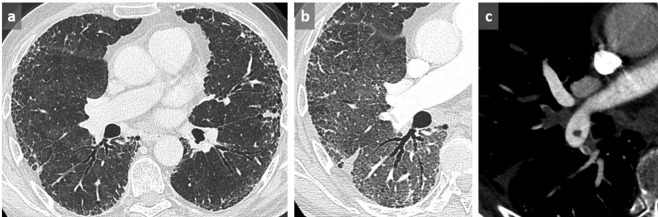
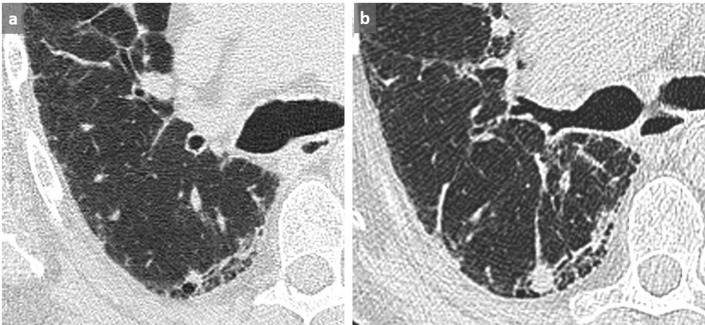
The diagnosis of interstitial lung disease may be challenging, especially in atypical disease. Various factors must be considered when performing and reading a chest CT examination for interstitial lung disease, because each of them may represent a source of misinterpretation. Firstly, technical aspects must be mastered, including acquisition and reconstruction parameters as well as post-processing. Secondly, mistakes in interpretation related to the inaccurate description of predominant features, potentially leading to false-positive findings, as well as satisfaction of search must be avoided. In all cases, clinical context, coexisting chest abnormalities and previous examinations must be integrated into the analysis to suggest the most appropriate differential diagnosis.
© 2019 The Authors. Published by the British Institute of Radiology.
Figures
References
Publication types
LinkOut - more resources
Full Text Sources
