

Non gastro-esophageal reflux disease related esophagitis: an overview with a histologic diagnostic approach
- PMID: 33179617
- PMCID: PMC7931579
- DOI: 10.32074/1591-951X-156
Non gastro-esophageal reflux disease related esophagitis: an overview with a histologic diagnostic approach
Abstract
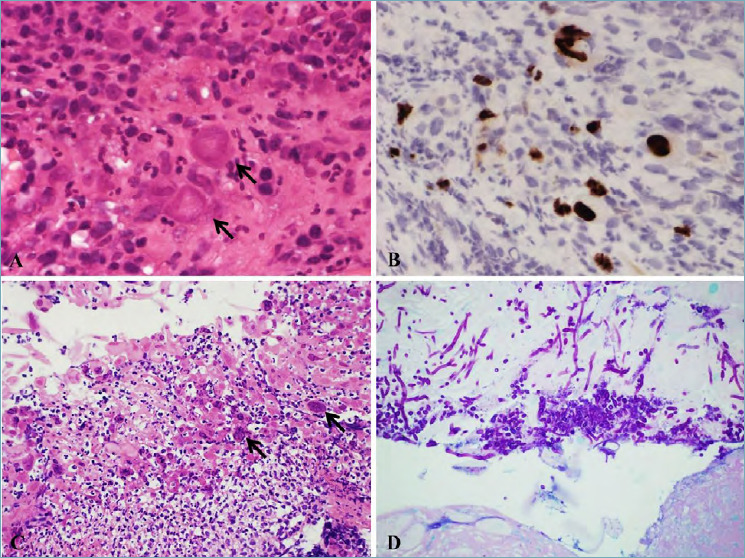
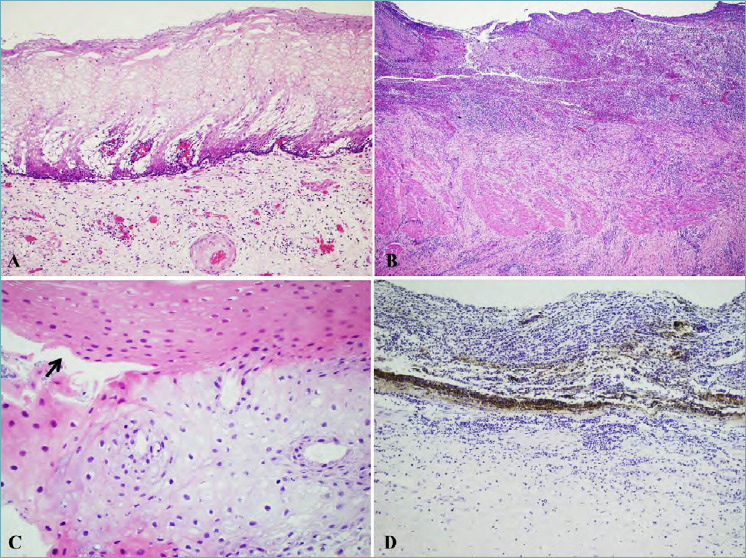
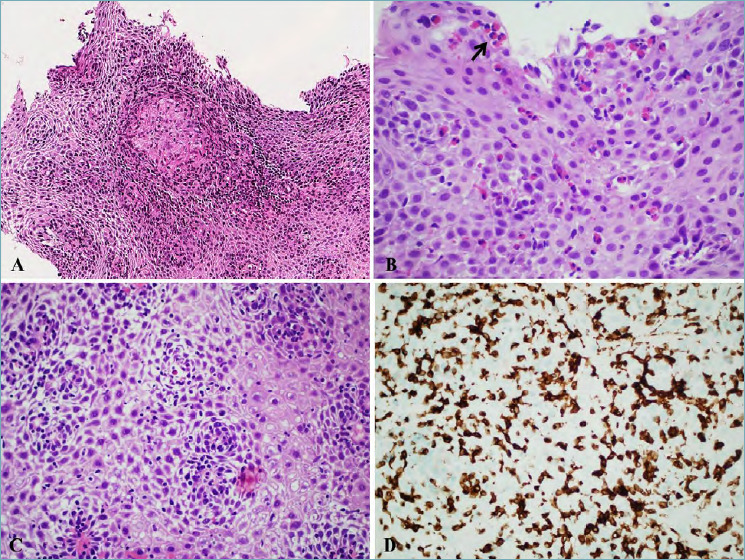
Several pathological conditions, other than gastro-esophageal reflux disease and its complications, can affect the esophagus. While some of these can present with unspecific lesions (i.e. ulcers and epithelial damage) and require clinico-pathological correlation for diagnosis (i.e. drug-induced esophagitis and corrosive esophagitis) other conditions show distinctive histological lesions which enable the pathologist to reach the diagnosis (i.e. some specific infectious esophagites and Crohn's disease). In this context eosinophilic esophagitis is the condition which has been increasingly studied in the last two decades, while lymphocytic esophagitis, a relatively new entity, still represents an enigma. This overview will focus on and describe histologic lesions which allow pathologists to differentiate between these conditions.
Keywords: drug-induced esophagitis; eosinophilic esophagitis; esophageal Crohn’s disease; esophagitis dissecans superficialis; lymphocytic esophagitis.
Copyright © 2020 Società Italiana di Anatomia Patologica e Citopatologia Diagnostica, Divisione Italiana della International Academy of Pathology.
Conflict of interest statement
The Authors declare no conflict of interest.
Figures
References
-
- Ahuja NK, Clarke JO. Evaluation and management of infectious esophagitis in immunocompromised and immunocompetent individuals. Curr Treat Options Gastro 2016;14:28-38. https://doi.org/10.1007/s11938-016-0082-2 10.1007/s11938-016-0082-2 - DOI - PubMed
-
- Mohamed AA, Lu XL, Mounmin FA. Diagnosis and treatment of esophageal candidiasis: current updates. Can J Gastroenterol Hepatol. 2019:3585136. https://doi.org/10.1155/2019/3585136 10.1155/2019/3585136 - DOI - PMC - PubMed
-
- Itoh T, Takahashi T, Kusaka K, et al. . Herpes simplex esophagitis from 1307 autopsy cases. J Gastroenterol Hepatol. 2003;18:1407-1411. https://doi.org/10.1046/j.1440-1746.2003.03166.x 10.1046/j.1440-1746.2003.03166.x - DOI - PubMed
-
- Wang HW, Kuo CJ, Lin WR, et al. . The clinical characteristics and manifestations of cytomegalovirus esophagitis. Dis Esophagus 2016;29:392-399. https://doi.org/10.1111/dote.12340 10.1111/dote.12340 - DOI - PubMed
-
- Maguire A, Sheahan K. Pathology of oesophagitis. Histopathology. 2012;60:864-879. https://doi.org/10.1111/j.1365-2559.2011.03855.x 10.1111/j.1365-2559.2011.03855.x - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous
