

Inflammatory and tumor-like lesions of the pancreas
- PMID: 33179622
- PMCID: PMC7931580
- DOI: 10.32074/1591-951X-168
Inflammatory and tumor-like lesions of the pancreas
Abstract
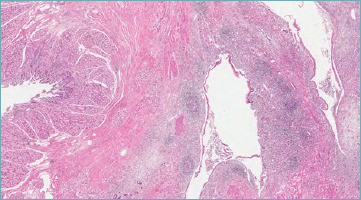
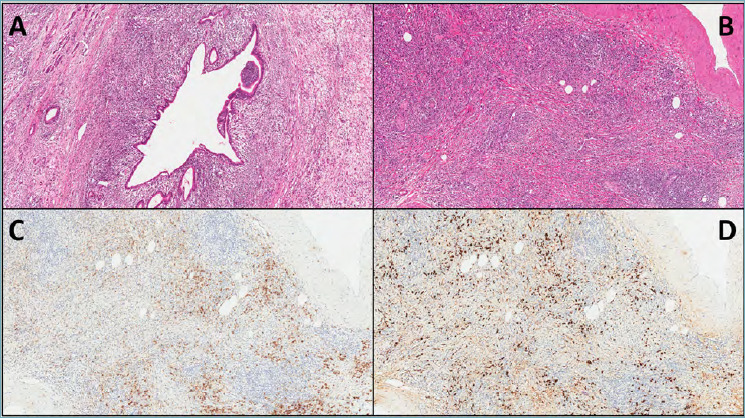
Inflammatory/tumor-like lesions of the pancreas represent a heterogeneous group of diseases that can variably involve the pancreatic gland determining different signs and symptoms. In the category of inflammatory/tumor-like lesions of the pancreas, the most important entities are represented by chronic pancreatitis, which includes alcoholic, obstructive and hereditary pancreatitis, paraduodenal (groove) pancreatitis, autoimmune pancreatitis, lymphoepithelial cyst, pancreatic hamartoma and intrapancreatic accessory spleen. An in-depth knowledge of such diseases is essential, since they can cause severe morbidity and may represent a potential life-threatening risk for patients. Furthermore, in some cases the differential diagnosis with malignant tumors may be challenging. Herein we provide a general overview of all these categories, with the specific aim of highlighting their most important clinic-pathological hallmarks to be used in routine diagnostic activities and clinical practice.
Keywords: autoimmune pancreatitis; chronic pancreatitis; groove; pancreatic pathology; paraduodenal pancreatitis.
Copyright © 2020 Società Italiana di Anatomia Patologica e Citopatologia Diagnostica, Divisione Italiana della International Academy of Pathology.
Conflict of interest statement
The Authors declare no conflict of interest.
Figures



Similar articles
-
Non-Neoplastic Masses of the Pancreas.Monogr Clin Cytol. 2020;26:42-52. doi: 10.1159/000455734. Epub 2020 Sep 28. Monogr Clin Cytol. 2020. PMID: 32987396 Review.
-
Benign Tumors and Tumorlike Lesions of the Pancreas.Surg Pathol Clin. 2016 Dec;9(4):619-641. doi: 10.1016/j.path.2016.05.007. Surg Pathol Clin. 2016. PMID: 27926363 Free PMC article. Review.
-
Paraduodenal pancreatitis: benign and malignant mimics at MRI.Abdom Radiol (NY). 2017 Nov;42(11):2652-2674. doi: 10.1007/s00261-017-1238-9. Abdom Radiol (NY). 2017. PMID: 28660333 Review.
-
Fine-needle aspiration features of paraduodenal pancreatitis (groove pancreatitis): a report of three cases.Diagn Cytopathol. 2012 Dec;40(12):1116-21. doi: 10.1002/dc.21722. Diagn Cytopathol. 2012. PMID: 21548125
-
A comprehensive, case-based review of groove pancreatitis.Pancreas. 2009 Aug;38(6):e169-75. doi: 10.1097/MPA.0b013e3181ac73f1. Pancreas. 2009. PMID: 19629001 Review.
Cited by
-
Imaging and histopathologic characteristics of typical pancreatic hamartoma: a case report and literature review.Front Oncol. 2024 Aug 19;14:1418244. doi: 10.3389/fonc.2024.1418244. eCollection 2024. Front Oncol. 2024. PMID: 39228982 Free PMC article.
-
Radiological Assessment After Pancreaticoduodenectomy for a Precision Approach to Managing Complications: A Narrative Review.J Pers Med. 2025 May 28;15(6):220. doi: 10.3390/jpm15060220. J Pers Med. 2025. PMID: 40559083 Free PMC article. Review.
-
The Rate of Avoidable Pancreatic Resections at a High-Volume Center: An Internal Quality Control and Critical Review.J Clin Med. 2023 Feb 17;12(4):1625. doi: 10.3390/jcm12041625. J Clin Med. 2023. PMID: 36836160 Free PMC article.
-
Surgery for chronic pancreatitis: the comparison of two high-volume centers reveals lack of a uniform operative management.Langenbecks Arch Surg. 2021 Dec;406(8):2669-2677. doi: 10.1007/s00423-021-02335-1. Epub 2021 Oct 1. Langenbecks Arch Surg. 2021. PMID: 34596765 Free PMC article.
-
Impact of tumor type and size on macroscopic tissue core retrieval in endoscopic ultrasound-guided fine needle biopsy for pancreatic malignancies.BMC Gastroenterol. 2024 Nov 19;24(1):415. doi: 10.1186/s12876-024-03517-z. BMC Gastroenterol. 2024. PMID: 39563255 Free PMC article.
References
-
- Stram M, Liu S, Singhi AD. Chronic pancreatitis. Surg Pathol Clin 2016;9:643-59. https://doi.org/10.1016/j.path.2016.05.008 10.1016/j.path.2016.05.008 - DOI - PubMed
-
- Etemad B, Whitcomb DC. Chronic pancreatitis: diagnosis, classification, and new genetic developments. Gastroenterology 2001;120:682-707. https://doi.org/10.1053/gast.2001.22586 10.1053/gast.2001.22586 - DOI - PubMed
-
- Lankisch PG, Assmus C, Maisonneuve P, et al. . Epidemiology of pancreatic diseases in Lüneburg County. A study in a defined german population. Pancreatology 2002;2:469-77. https://doi.org/10.1159/000064713 10.1159/000064713 - DOI - PubMed
-
- Lowenfels AB, Maisonneuve P, Cavallini G, et al. . Pancreatitis and the risk of pancreatic cancer. International Pancreatitis Study Group. N Engl J Med 1993;328(20):1433-7. https://doi.org/10.1056/NEJM199305203282001 10.1056/NEJM199305203282001 - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
